Endoscopy Subscore=0
For moderate to severe ulcerative colitis (UC) in adult TNFi-IR patients.1
RINVOQ HELPS DELIVER
LONG-TERM
REMISSION DATA IN UC1
INDICATION
RINVOQ is indicated for the treatment of adults with moderately to severely active ulcerative colitis (UC) who have had an inadequate response or intolerance to one or more tumor necrosis factor (TNF) blockers. If TNF blockers are clinically inadvisable, patients should have received at least one approved systemic therapy prior to use of RINVOQ.
Limitations of Use: RINVOQ is not recommended for use in combination with other Janus kinase (JAK) inhibitors, biological therapies for UC, or with potent immunosuppressants such as azathioprine and cyclosporine.
Durable Remission1,2
Clinical remission* at Week 8 and Week 521
Remission data observed at Week 1482†
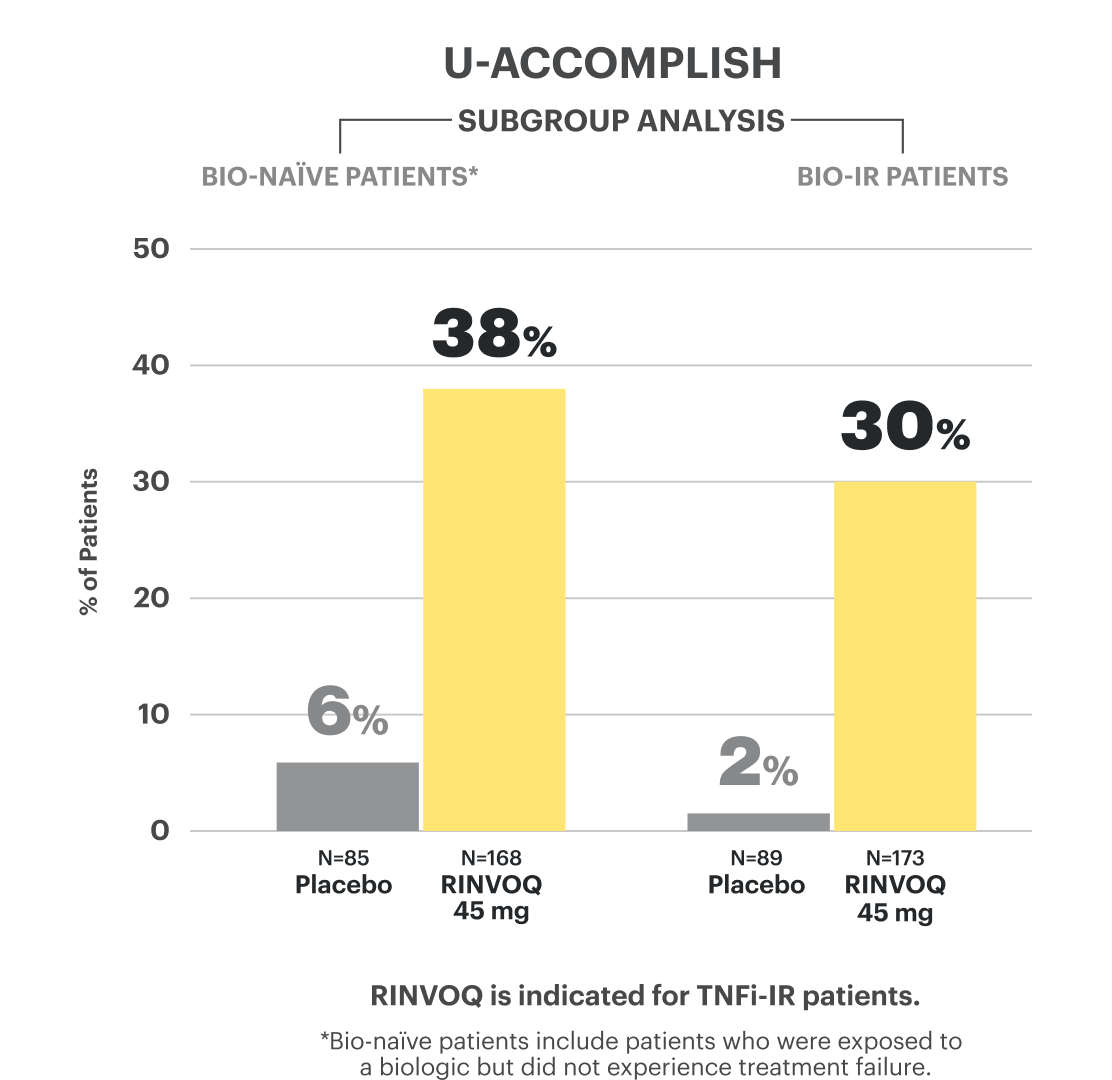
Bio-IR‡ data available at Week 52 and at Week 1481,2†
†Based on not statistically significant data. No conclusions can be made.
Powerful Healing1,2
Endoscopic improvement§ and histo-endoscopic mucosal improvement||¶ at Week 8 and Week 521
Endoscopic data observed at Week 1482†
Bio-IR‡ data available at Week 52 and at Week 1481,2†
†Based on not statistically significant data. No conclusions can be made.
¶The relationship between histo-endoscopic mucosal improvement to disease progression and long-term outcomes was not evaluated.
Rapid Relief1
Rapid relief of rectal bleeding and stool frequency at Week 2#
*Clinical remission per modified Mayo Score is defined as stool frequency subscore ≤1 and not greater than baseline, rectal bleeding subscore of 0, and endoscopic subscore ≤1 without friability.
‡Bio-IR is defined as patients who have an inadequate response to, lose response to, or are intolerant to biologic therapy.
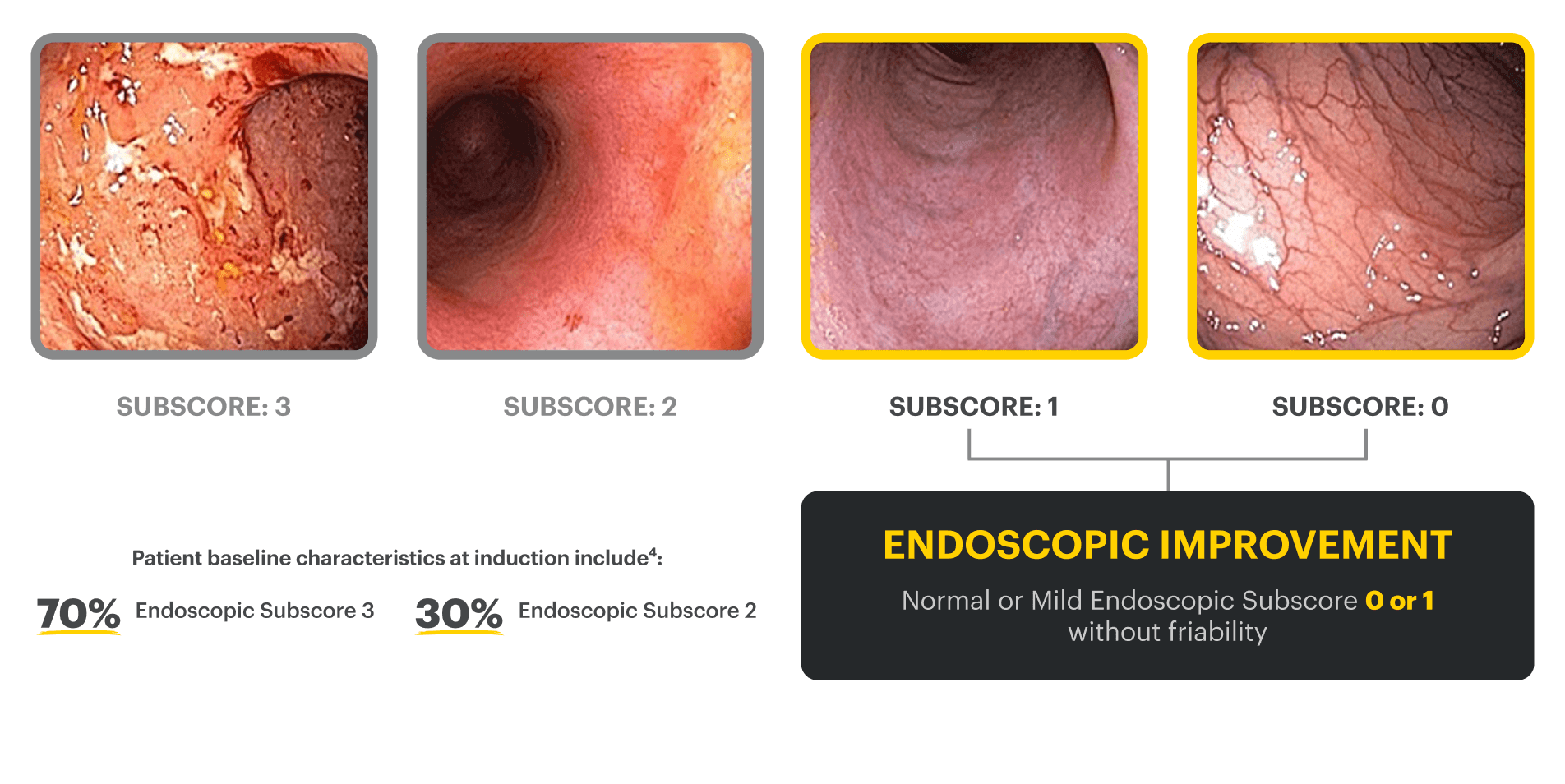
§Endoscopic improvement was defined as Mayo endoscopic subscore of 0 or 1 without friability. Endoscopic results are based on a full colonoscopy or flexible sigmoidoscopy, depending on the extent of disease at study entry.
||Histo-endoscopic mucosal improvement was defined as Mayo endoscopy subscore of 0 or 1 without friability and Geboes score ≤3.1 (neutrophil infiltration in <5% of crypts, no crypt destruction, and no erosions, ulcerations, or granulation tissue). Endoscopic results are based on a full colonoscopy or flexible sigmoidoscopy, depending on the extent of disease at study entry, and histology results are based on a set of 2 biopsies.
#Clinical response per partial modified Mayo Score is a composite of Mayo stool frequency and rectal bleeding subscores and is defined as a decrease in total score ≥30% and ≥1 point from baseline and a decrease in rectal bleeding subscore ≥1 or rectal bleeding subscore of 0 or 1.
IR=intolerance or inadequate response; TNFi=tumor necrosis factor inhibitor.
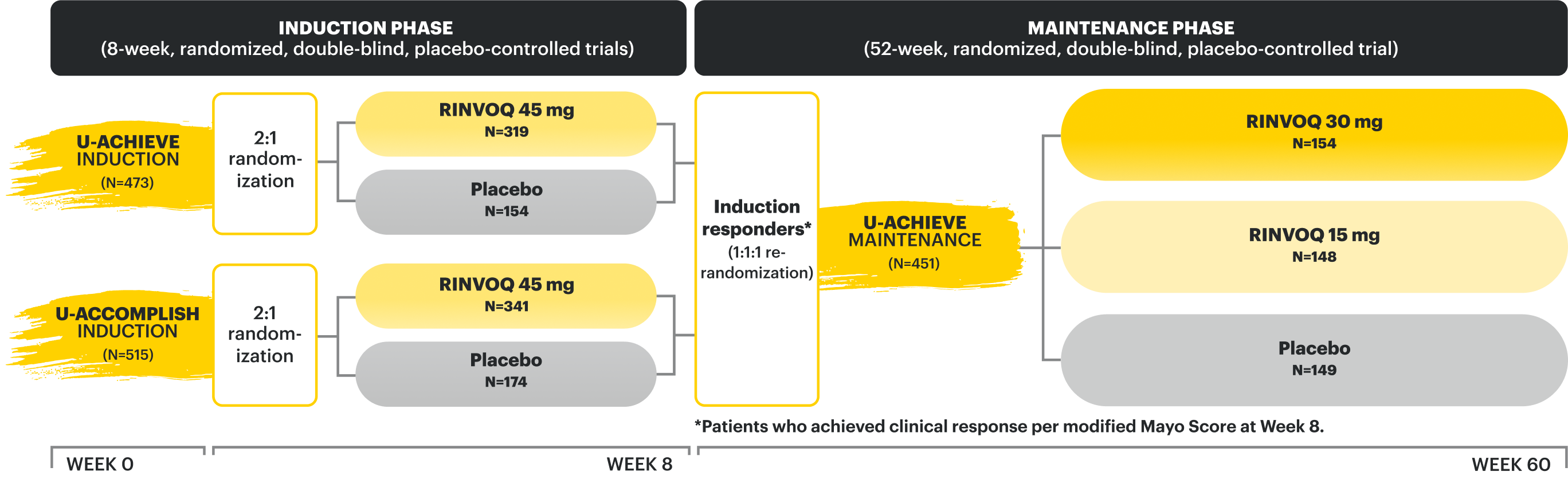
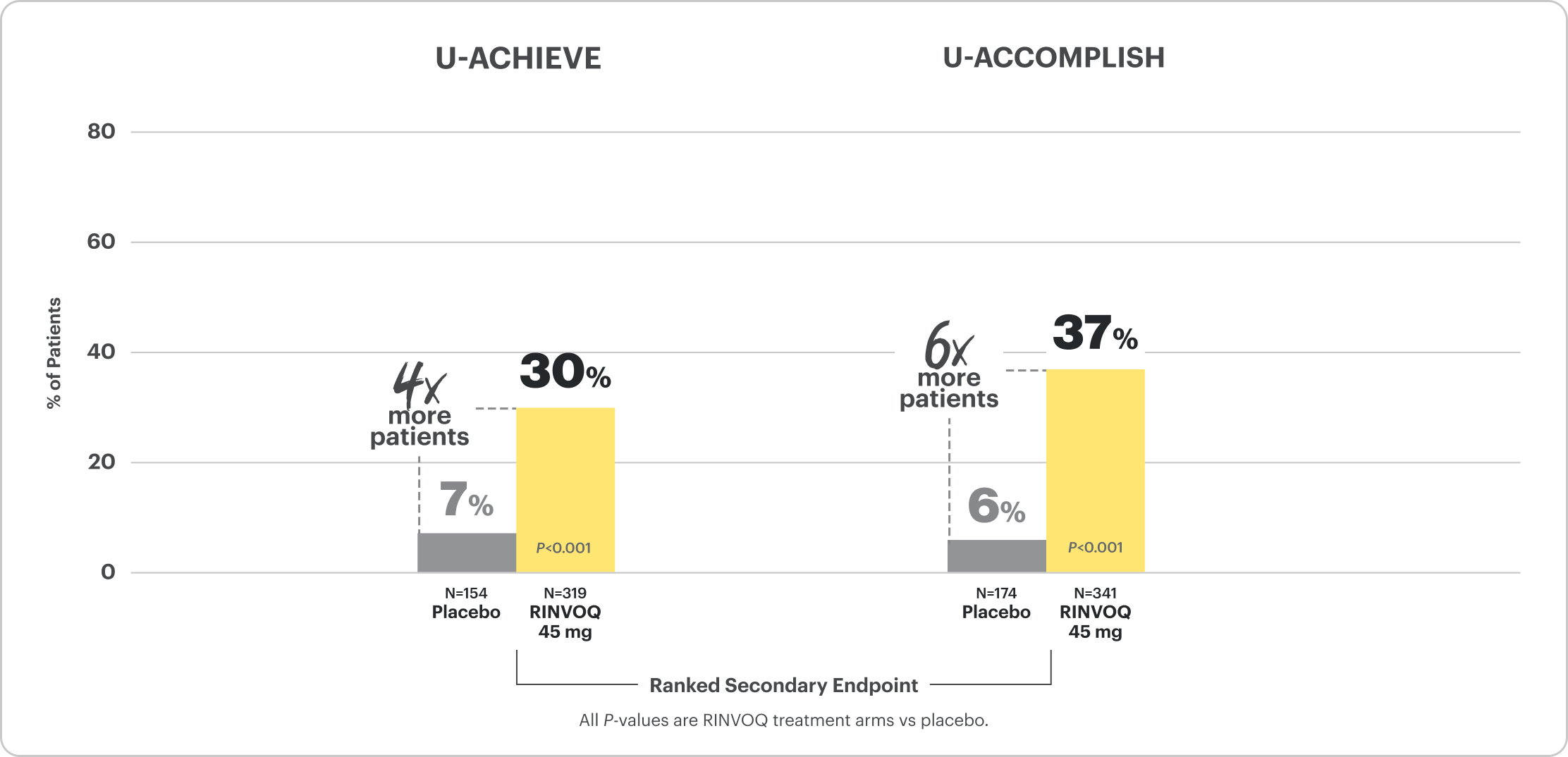
U-ACHIEVE Induction and U-ACCOMPLISH Induction Study Design Intro1: 8-week, double-blind, placebo-controlled, Phase 3 clinical studies of 988 patients (473 patients for U-ACHIEVE and 515 patients for U-ACCOMPLISH) with moderately to severely active UC and demonstrated prior treatment failure to oral aminosalicylates, corticosteroids, immunosuppressants, and/or biologic treatment. Patients were randomized to receive either RINVOQ 45 mg or placebo once daily for 8 weeks. The primary endpoint was clinical remission per modified Mayo Score at Week 8.
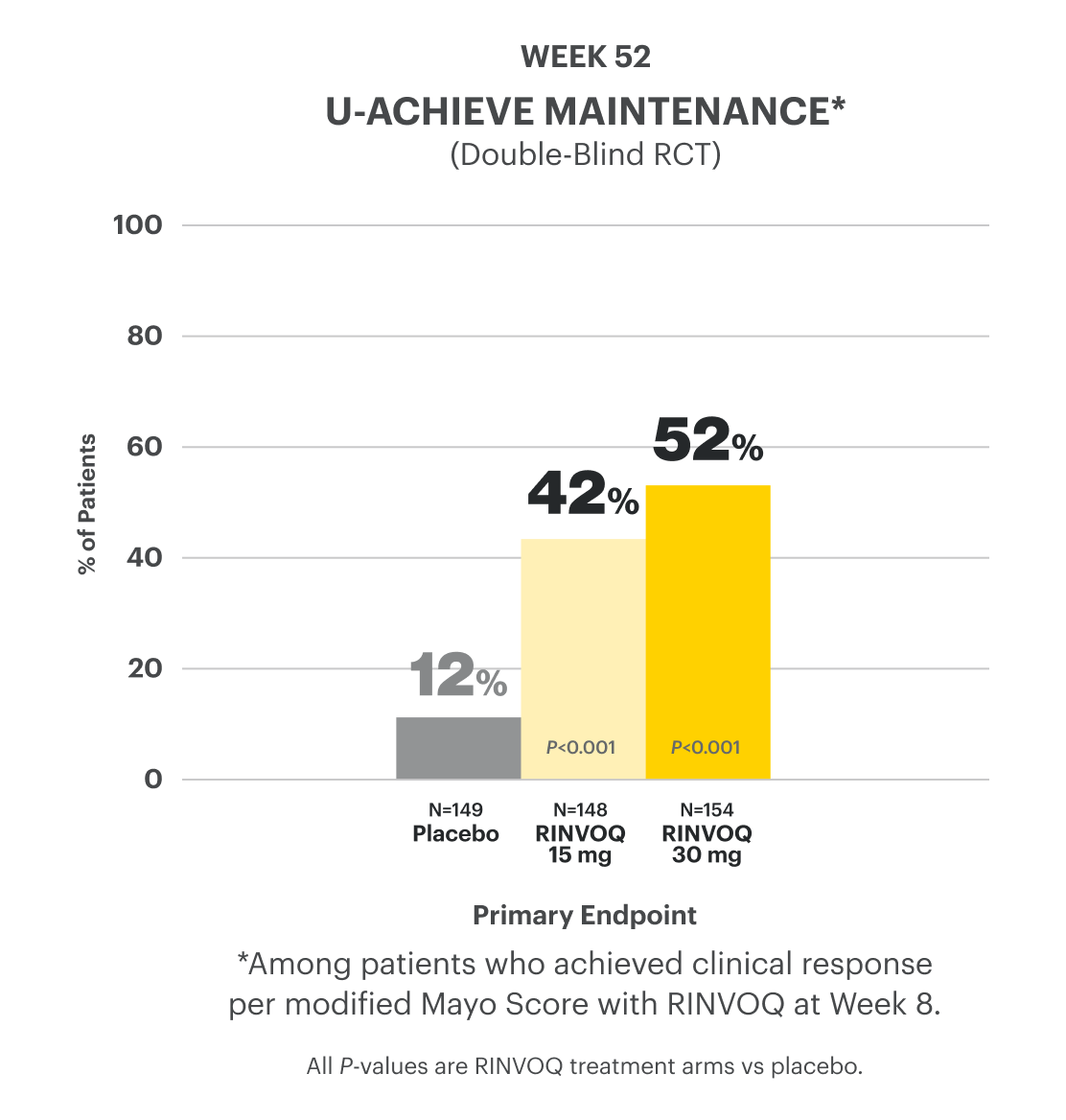
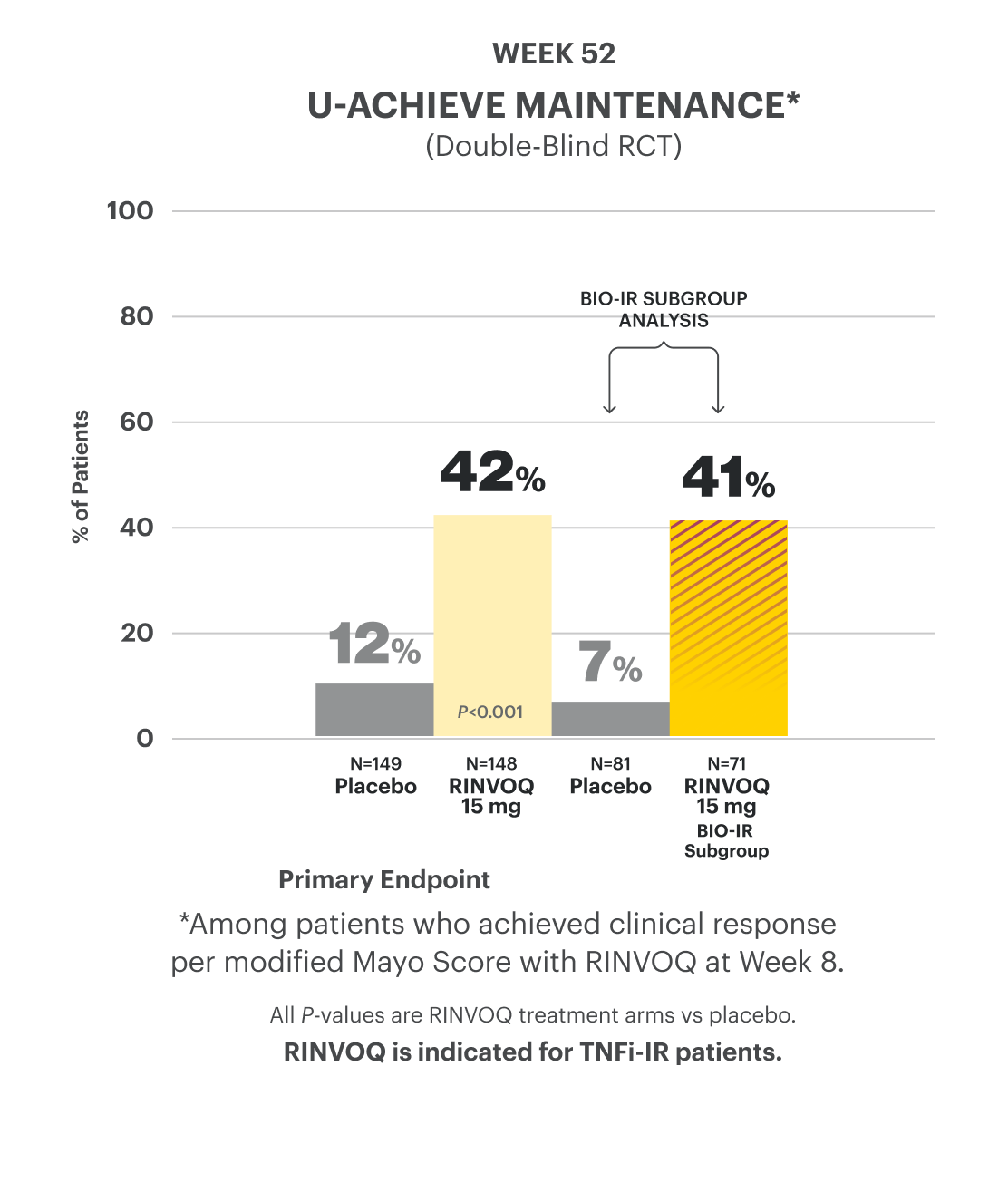
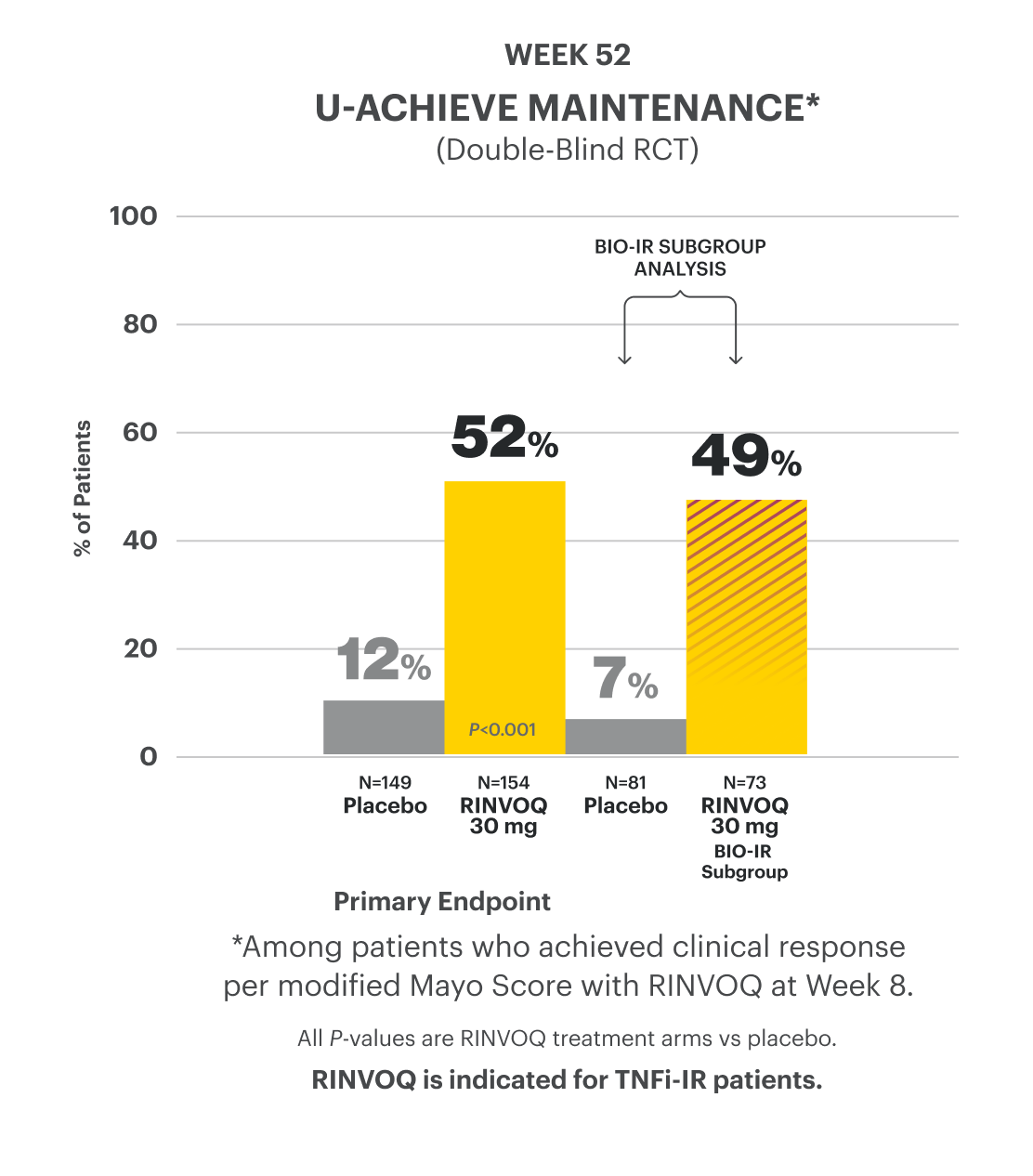
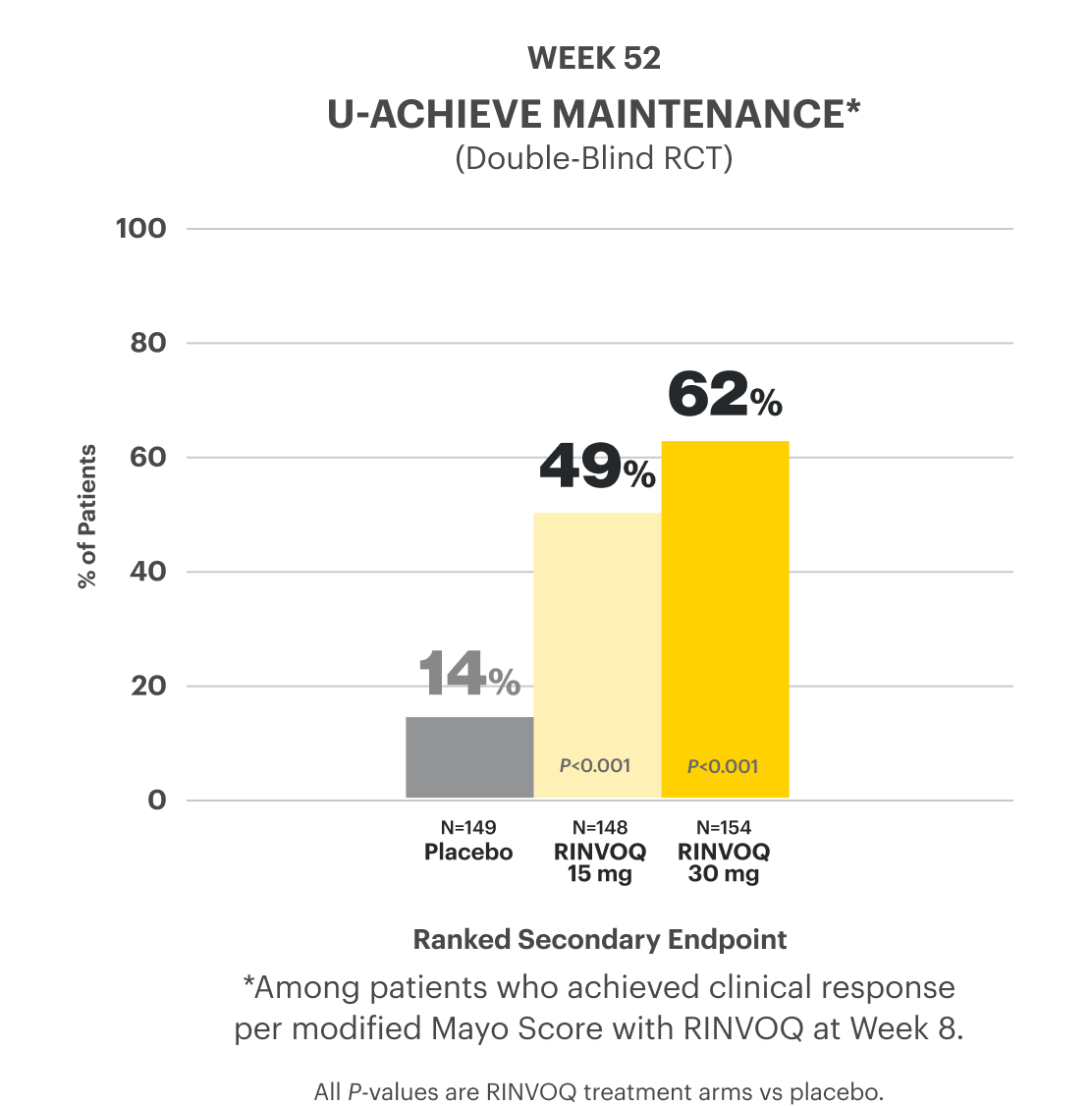
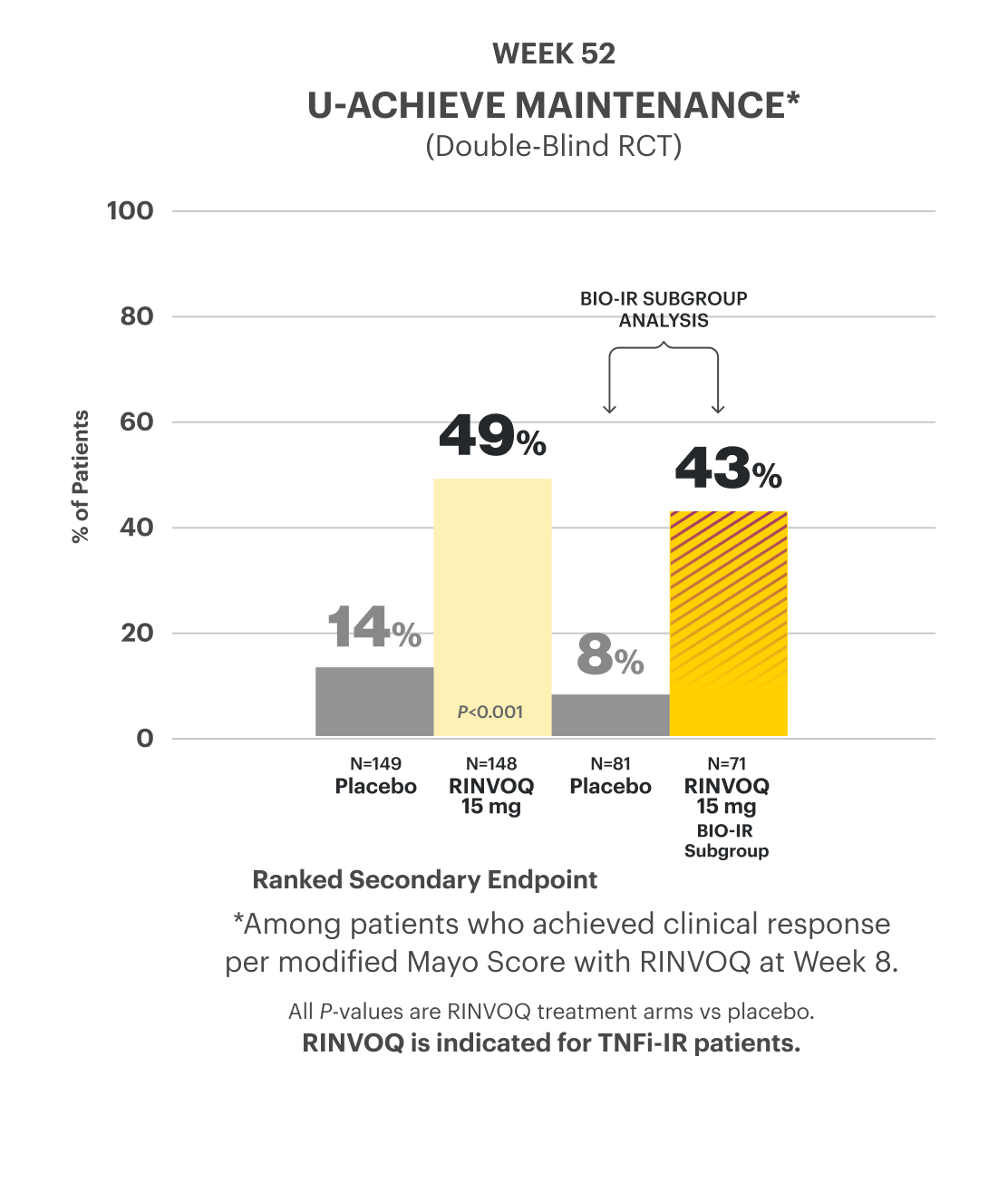
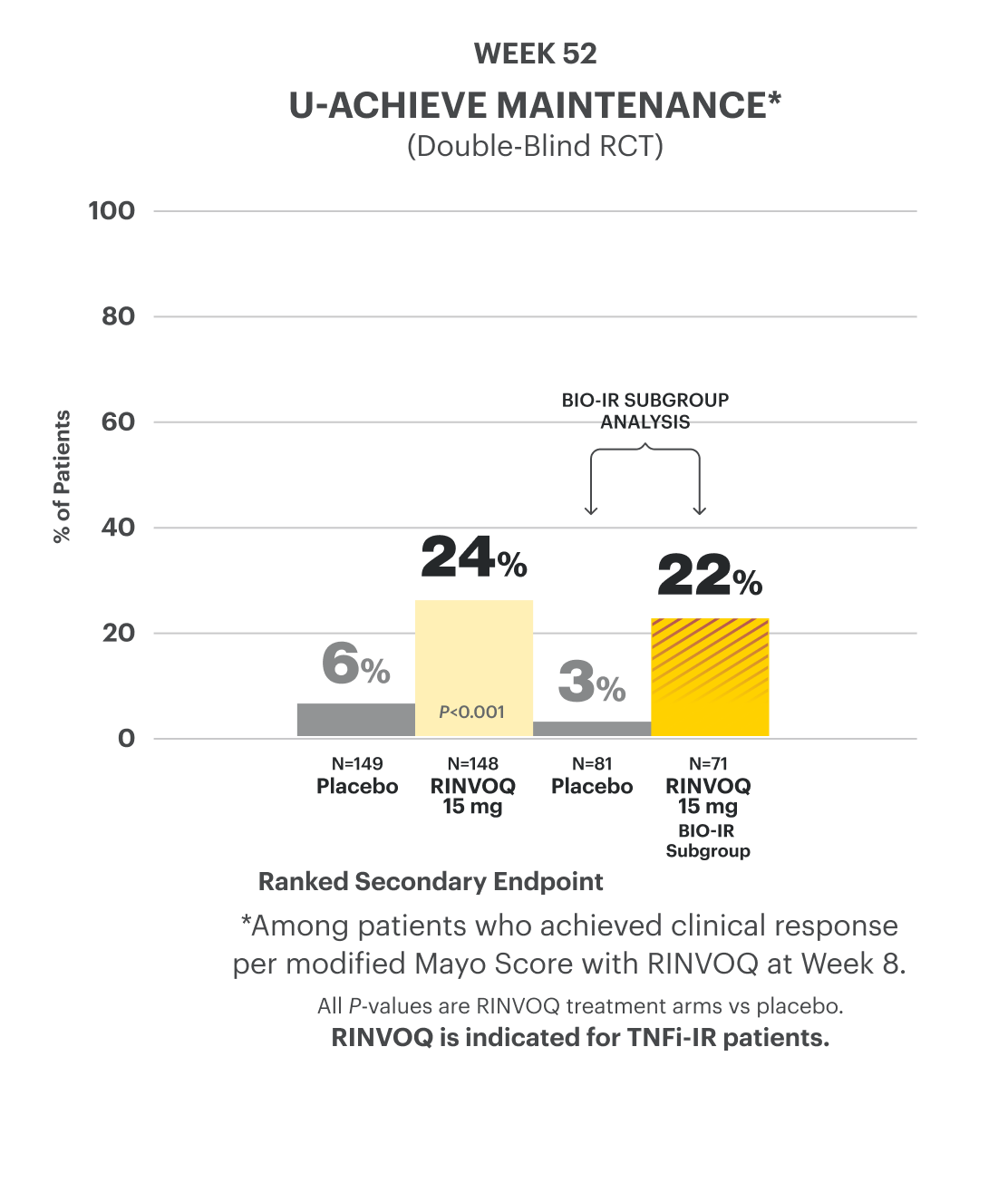
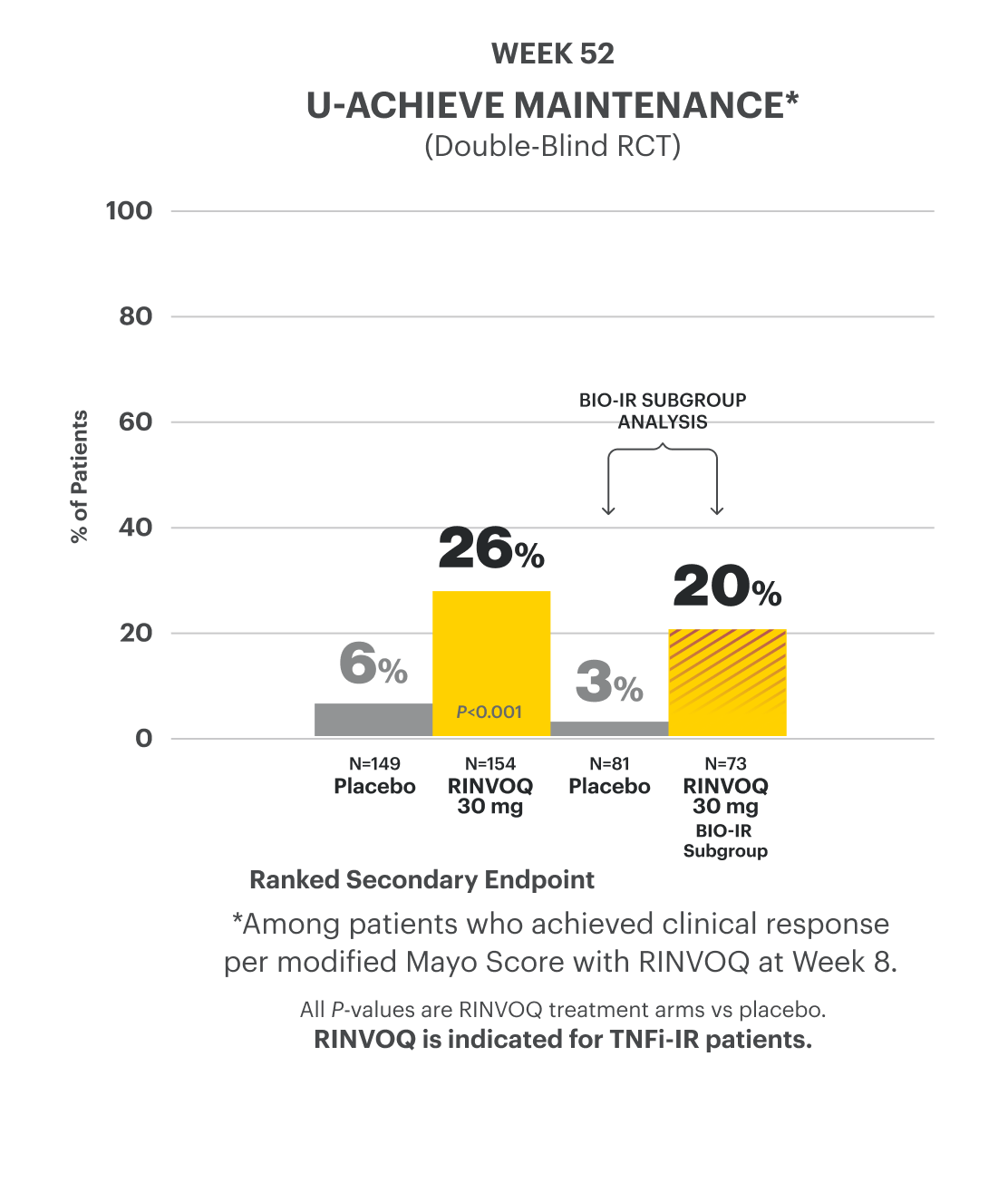
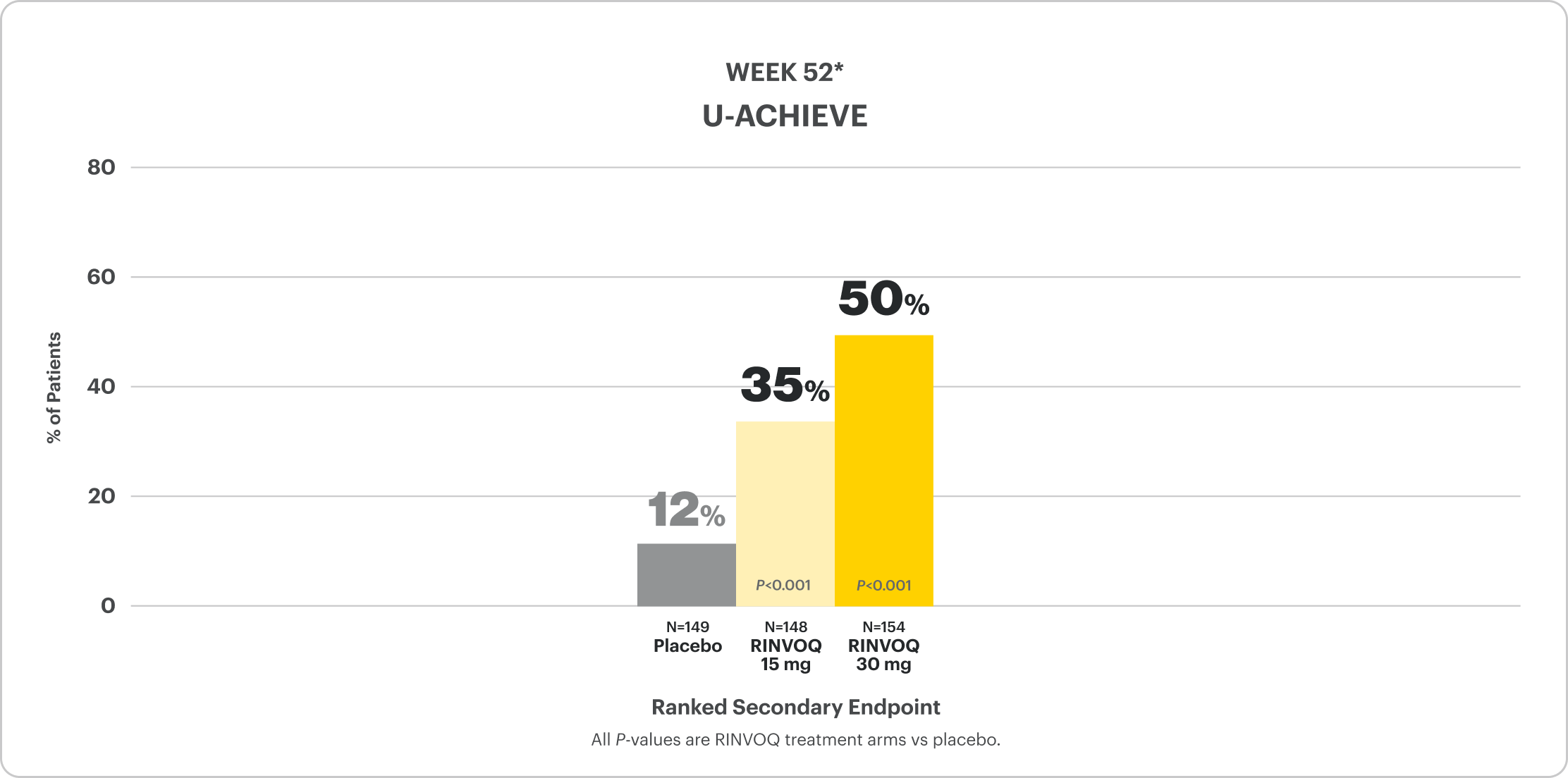
U-ACHIEVE Maintenance Study Design Intro1: 52-week, double-blind, placebo-controlled, Phase 3 clinical study of 746 patients who achieved clinical response per modified Mayo Score (a decrease in total score ≥30% and ≥2 points from baseline and a decrease in rectal bleeding subscore ≥1 or rectal bleeding subscore of 0 or 1) during induction with 8-week RINVOQ 45 mg once daily and were re-randomized to the maintenance study. The primary efficacy analysis population was the first randomized 451 patients. Patients were randomized to receive RINVOQ 15 mg, 30 mg, or placebo once daily for up to 52 weeks. The primary endpoint was clinical remission per modified Mayo Score at Week 52.
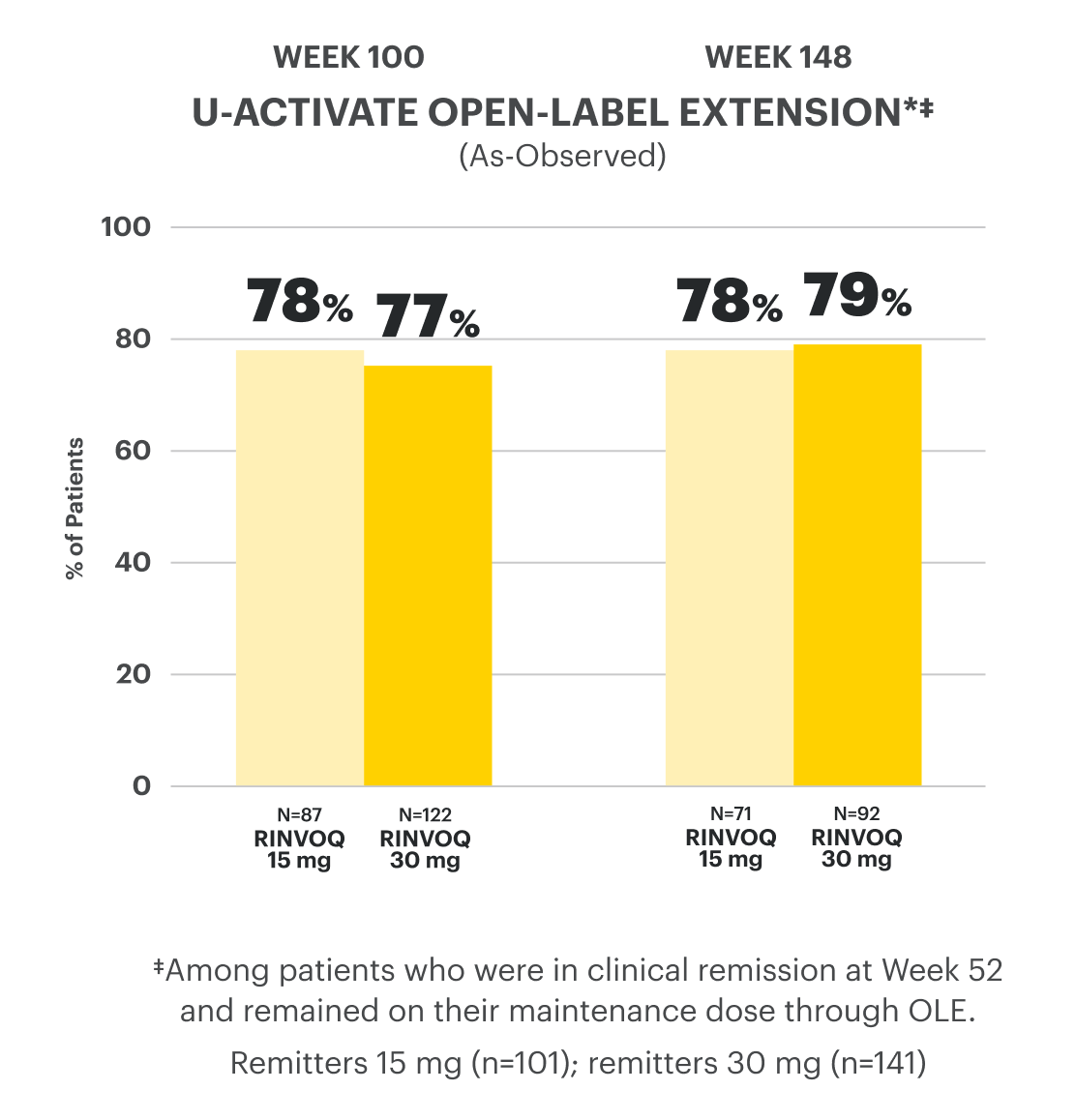
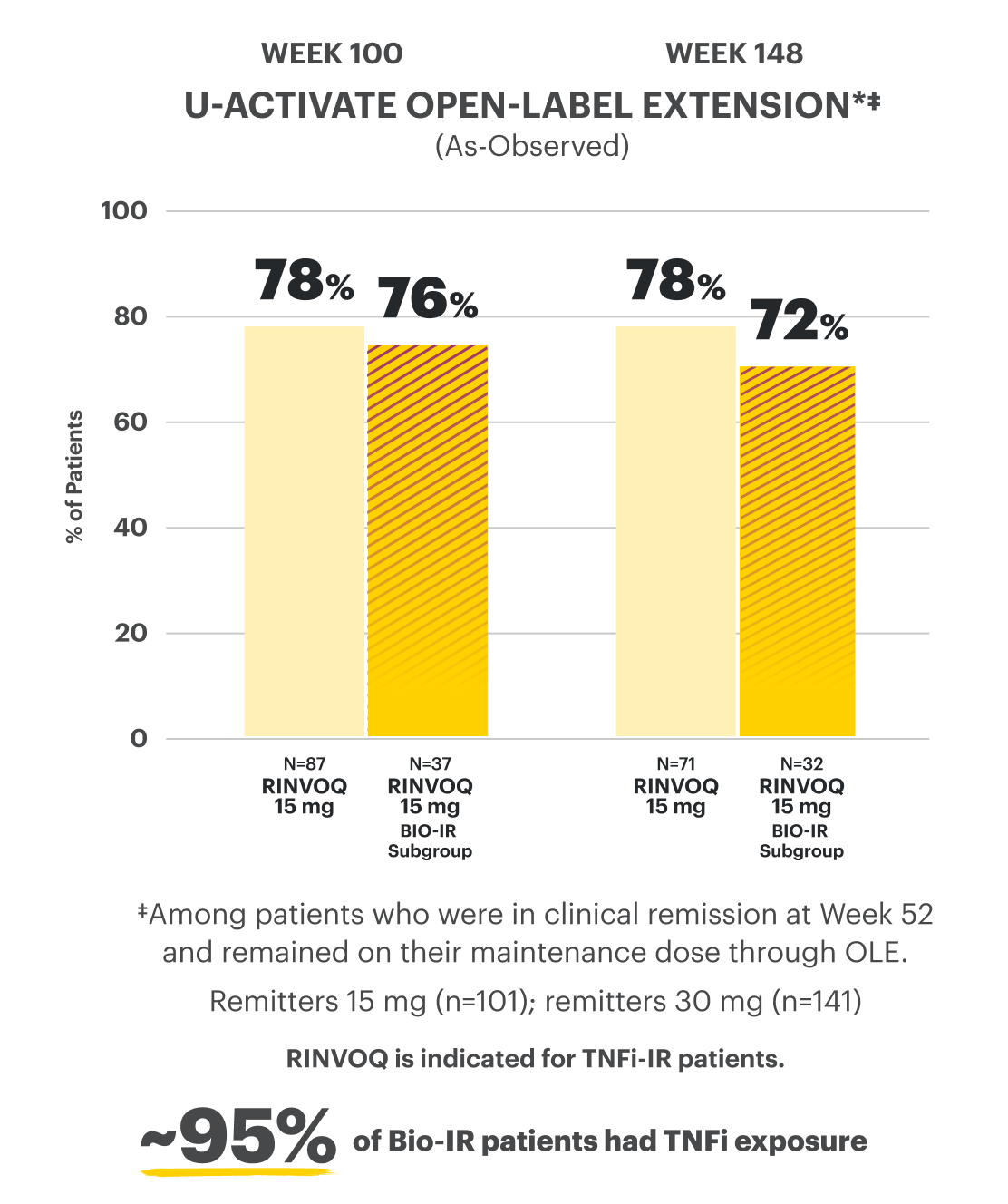
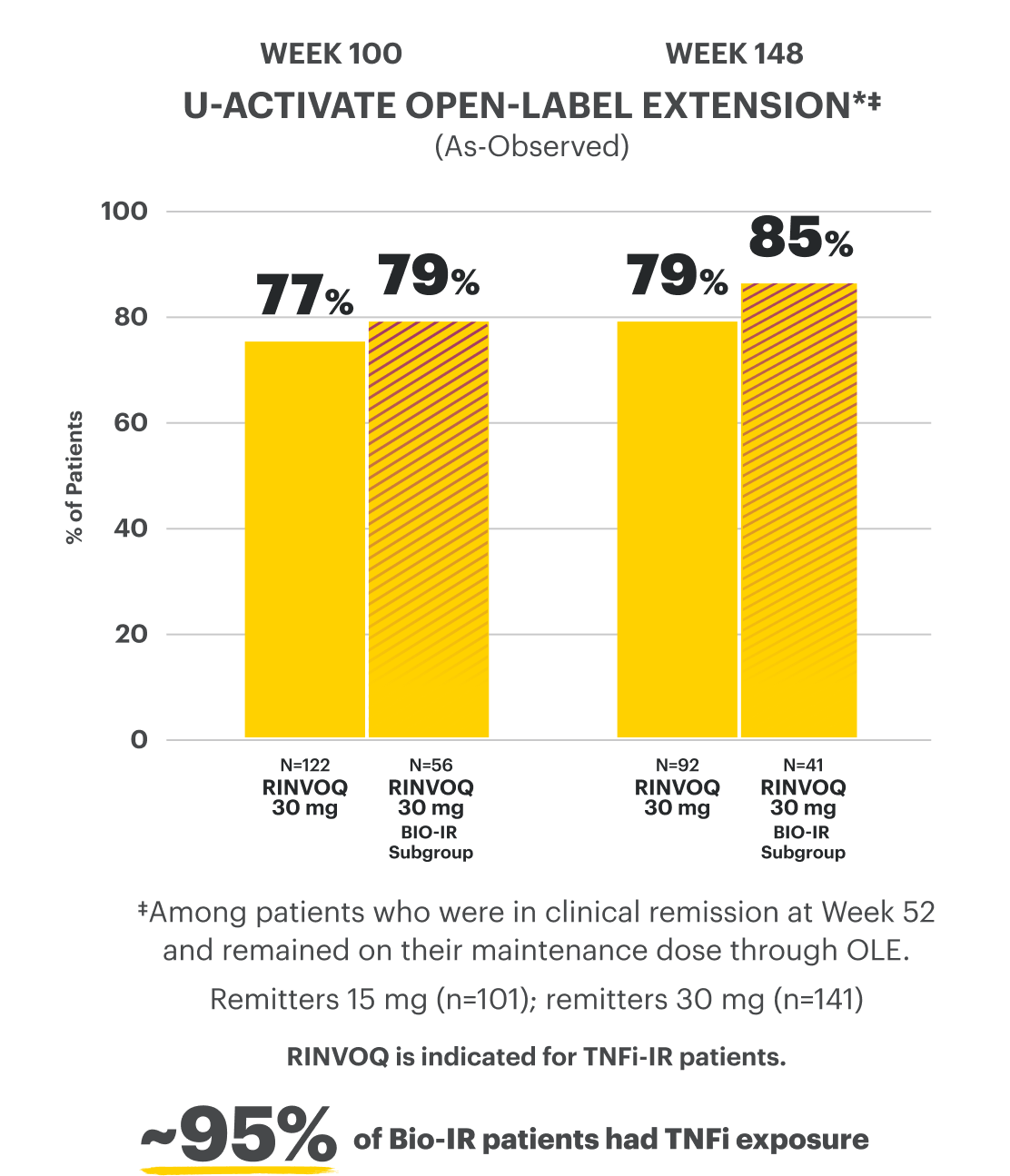
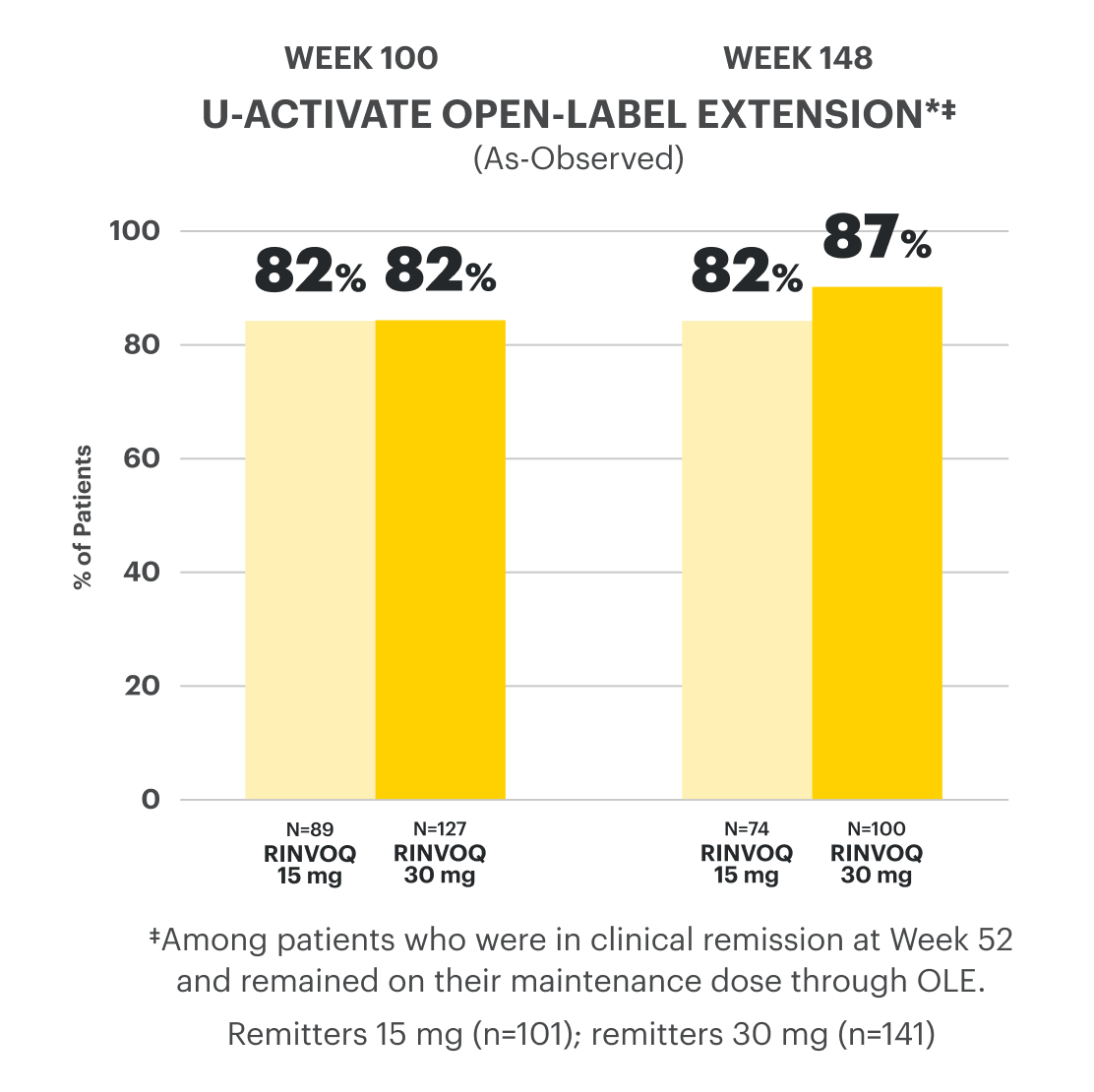
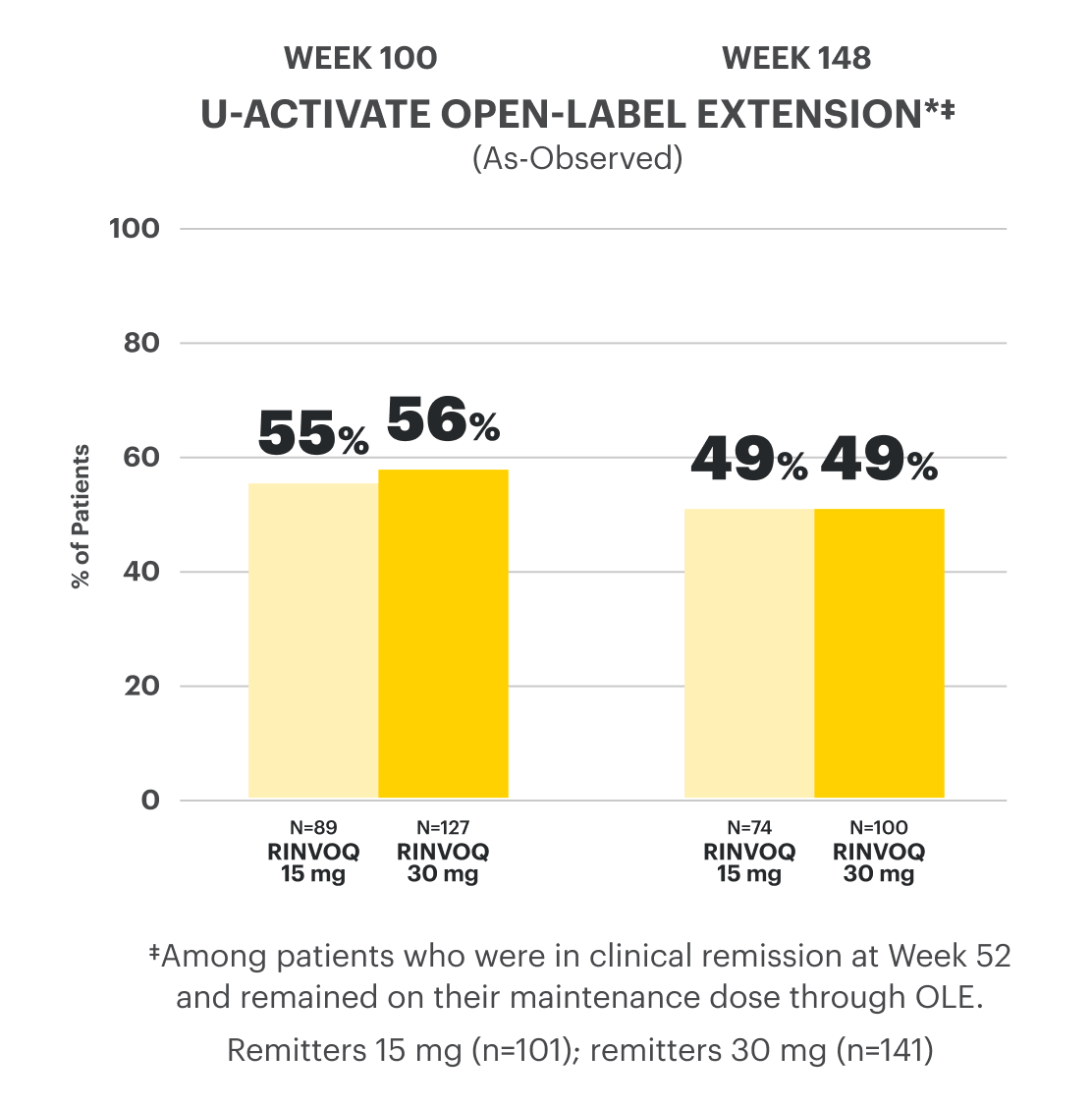
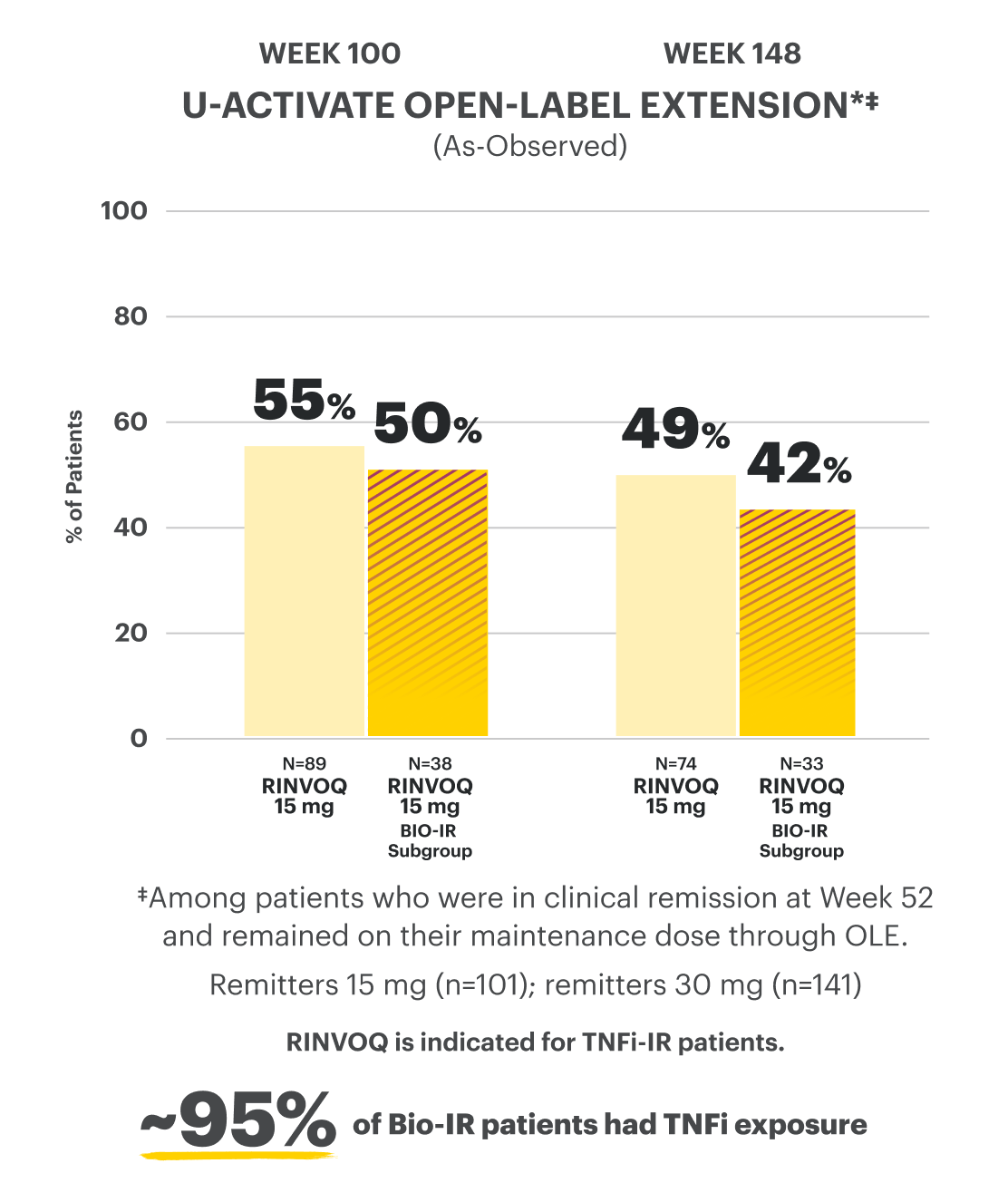
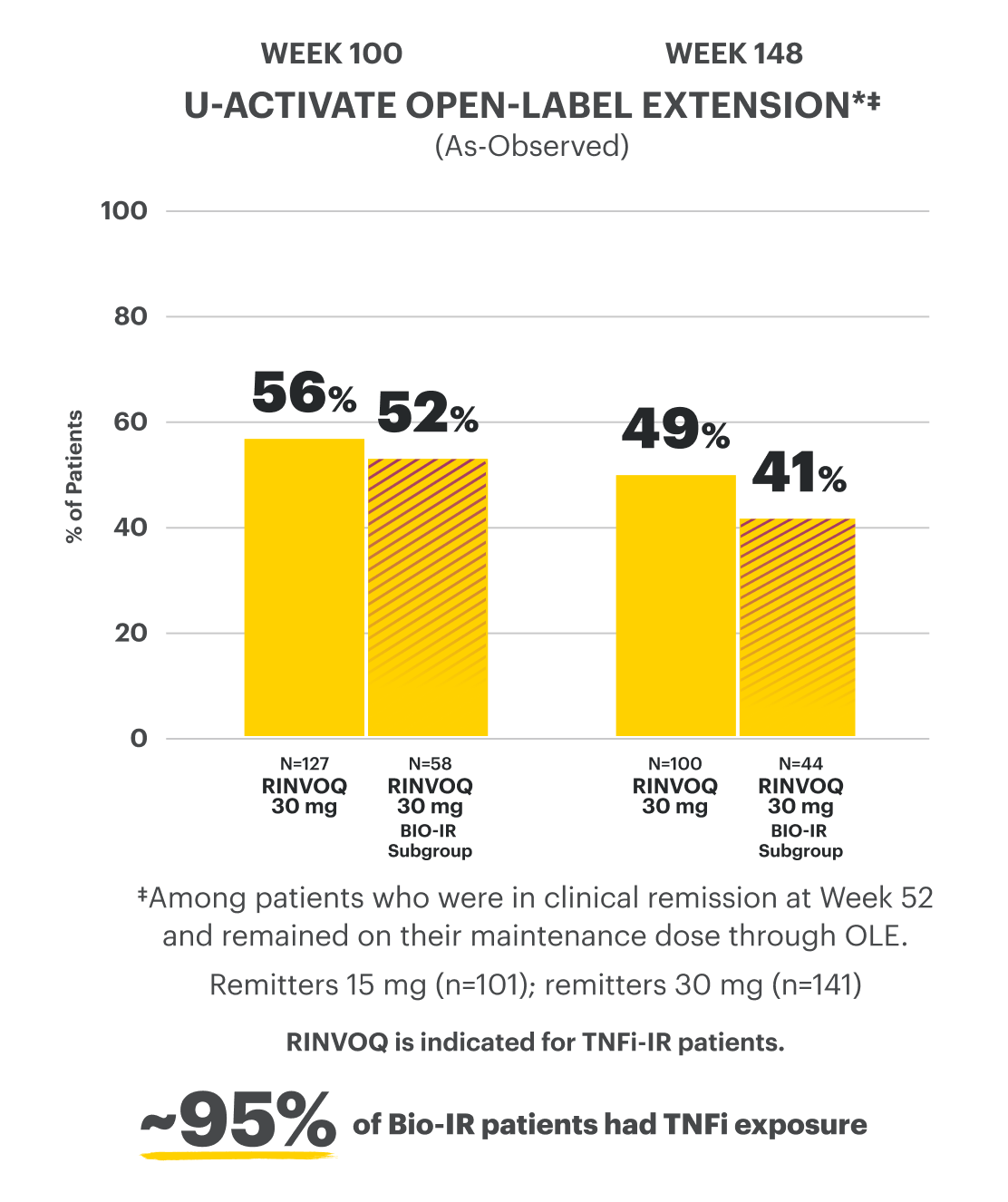
U-ACTIVATE Long-Term Extension (LTE) Open-Label Study2: Data presented at approximately 3 years is an interim analysis at 96 weeks of the U-ACTIVATE study, which is an ongoing 288-week, long-term study evaluating the efficacy and safety from patients who come from the U-ACHIEVE trial. Analysis includes patients from both primary (n=451) and full Maintenance populations (n=681). At the time of analysis, not all patients have reached 96 weeks of the LTE study.
In the LTE analysis, the data was segmented into 2 groups:
- RINVOQ 15 mg arm: Patients who achieved clinical remission (remitters) on RINVOQ 15 mg at Week 52 of Maintenance Trial and received continuous RINVOQ 15 mg in LTE period (n=101)
- RINVOQ 30 mg arm: Patients who achieved clinical remission (remitters) on RINVOQ 30 mg at Week 52 of Maintenance Trial and received continuous RINVOQ 30 mg in LTE period (n=141)
Please see Important Safety Information, including BOXED WARNING on Serious Infections, Mortality, Malignancies, Major Adverse Cardiovascular Events, and Thrombosis, below.
Durable Remission
at Weeks 8 and 52
Clinical Remission
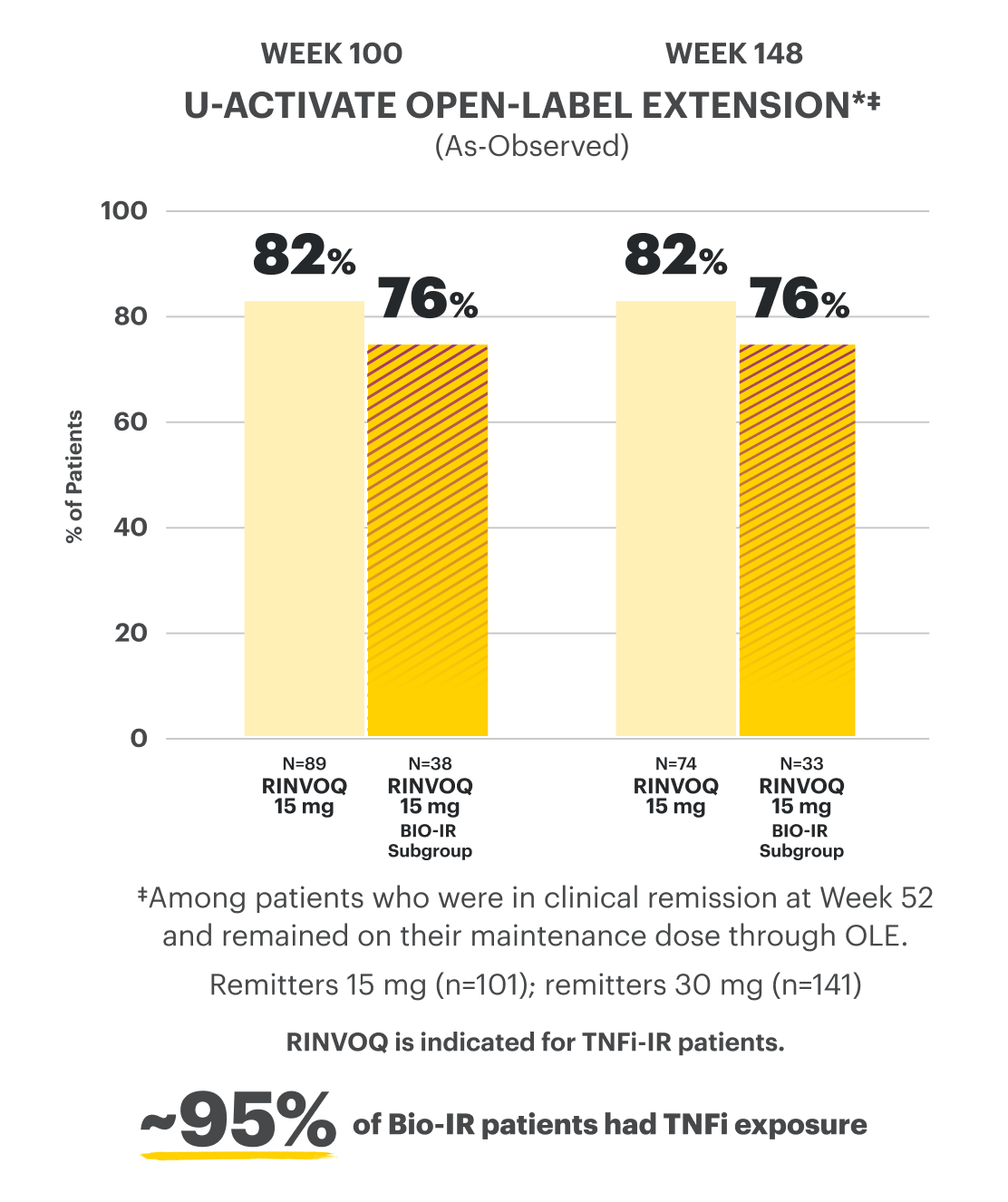
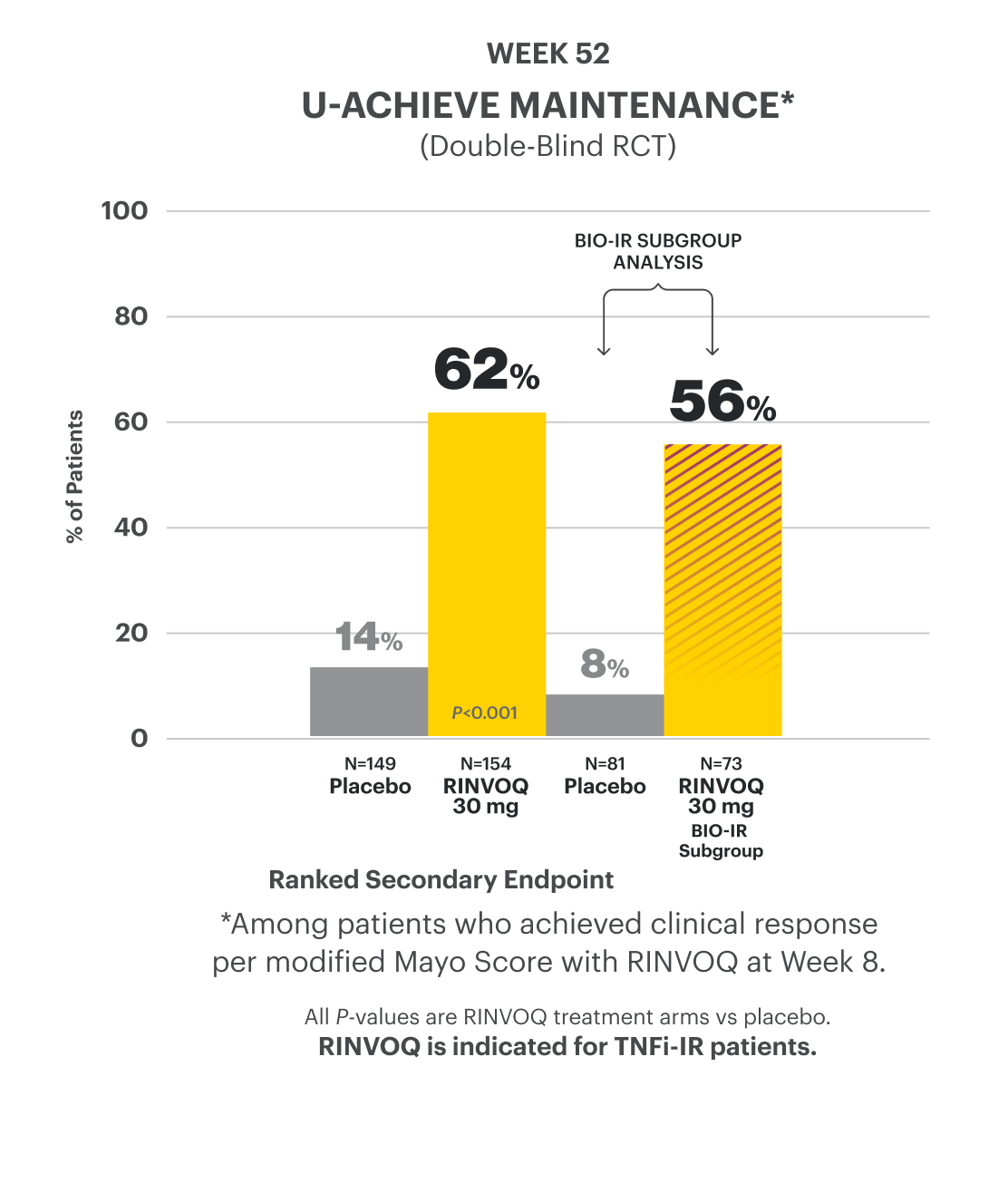
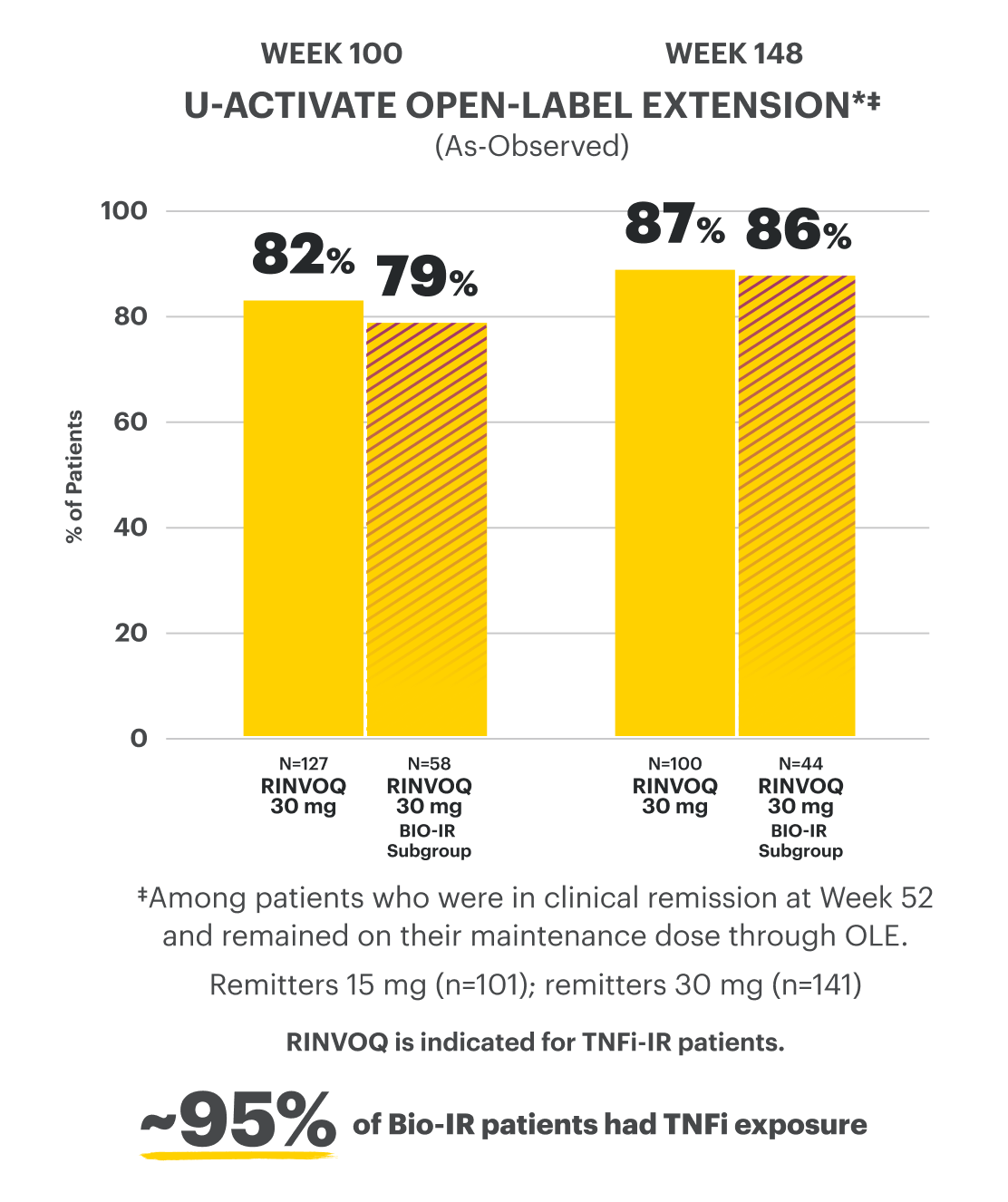
Clinical Remission at Week 52 and Up to Week 1481,2
(Composite of Rectal Bleeding, Stool Frequency, and Endoscopy Subscores)
RECOMMENDED MAINTENANCE DOSING
The recommended maintenance dosage of RINVOQ is 15 mg once daily. A dose of 30 mg once daily may be considered for patients with refractory, severe, or extensive disease. Discontinue RINVOQ if an adequate therapeutic response is not achieved with the 30 mg dose.
OLE LIMITATIONS: In an open-label extension (OLE), there is a potential for enrichment of the long-term data in the remaining patient populations since patients who are unable to tolerate or do not respond to the drug often drop out.
AO DISCLOSURE: In an as-observed (AO) analysis, missing visit data were excluded from calculations for that visit, which may increase the percent of responders. All observed data were used regardless of premature discontinuation of study drug or initiation of concomitant medications. The same patient may not have a response at each timepoint.
†Bio-IR is defined as patients who have an inadequate response to, lose response to, or are intolerant to biologic therapy.
RECOMMENDED MAINTENANCE DOSING
The recommended maintenance dosage of RINVOQ is 15 mg once daily. A dose of 30 mg once daily may be considered for patients with refractory, severe, or extensive disease. Discontinue RINVOQ if an adequate therapeutic response is not achieved with the 30 mg dose.
OLE LIMITATIONS: In an open-label extension (OLE), there is a potential for enrichment of the long-term data in the remaining patient populations since patients who are unable to tolerate or do not respond to the drug often drop out.
AO DISCLOSURE: In an as-observed (AO) analysis, missing visit data were excluded from calculations for that visit, which may increase the percent of responders. All observed data were used regardless of premature discontinuation of study drug or initiation of concomitant medications. The same patient may not have a response at each timepoint.
†Bio-IR is defined as patients who have an inadequate response to, lose response to, or are intolerant to biologic therapy.
RECOMMENDED MAINTENANCE DOSING
The recommended maintenance dosage of RINVOQ is 15 mg once daily. A dose of 30 mg once daily may be considered for patients with refractory, severe, or extensive disease. Discontinue RINVOQ if an adequate therapeutic response is not achieved with the 30 mg dose.
OLE LIMITATIONS: In an open-label extension (OLE), there is a potential for enrichment of the long-term data in the remaining patient populations since patients who are unable to tolerate or do not respond to the drug often drop out.
AO DISCLOSURE: In an as-observed (AO) analysis, missing visit data were excluded from calculations for that visit, which may increase the percent of responders. All observed data were used regardless of premature discontinuation of study drug or initiation of concomitant medications. The same patient may not have a response at each timepoint.
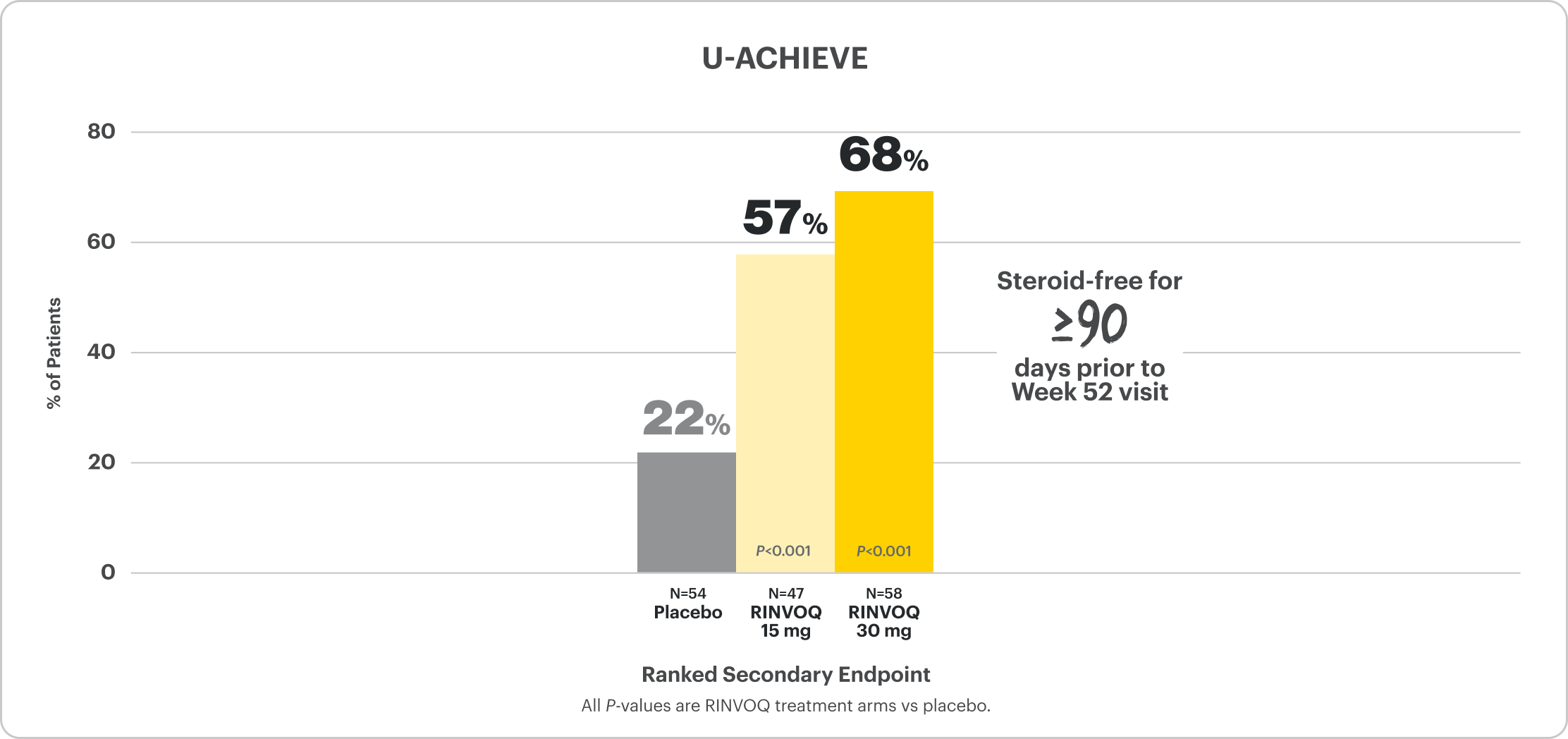
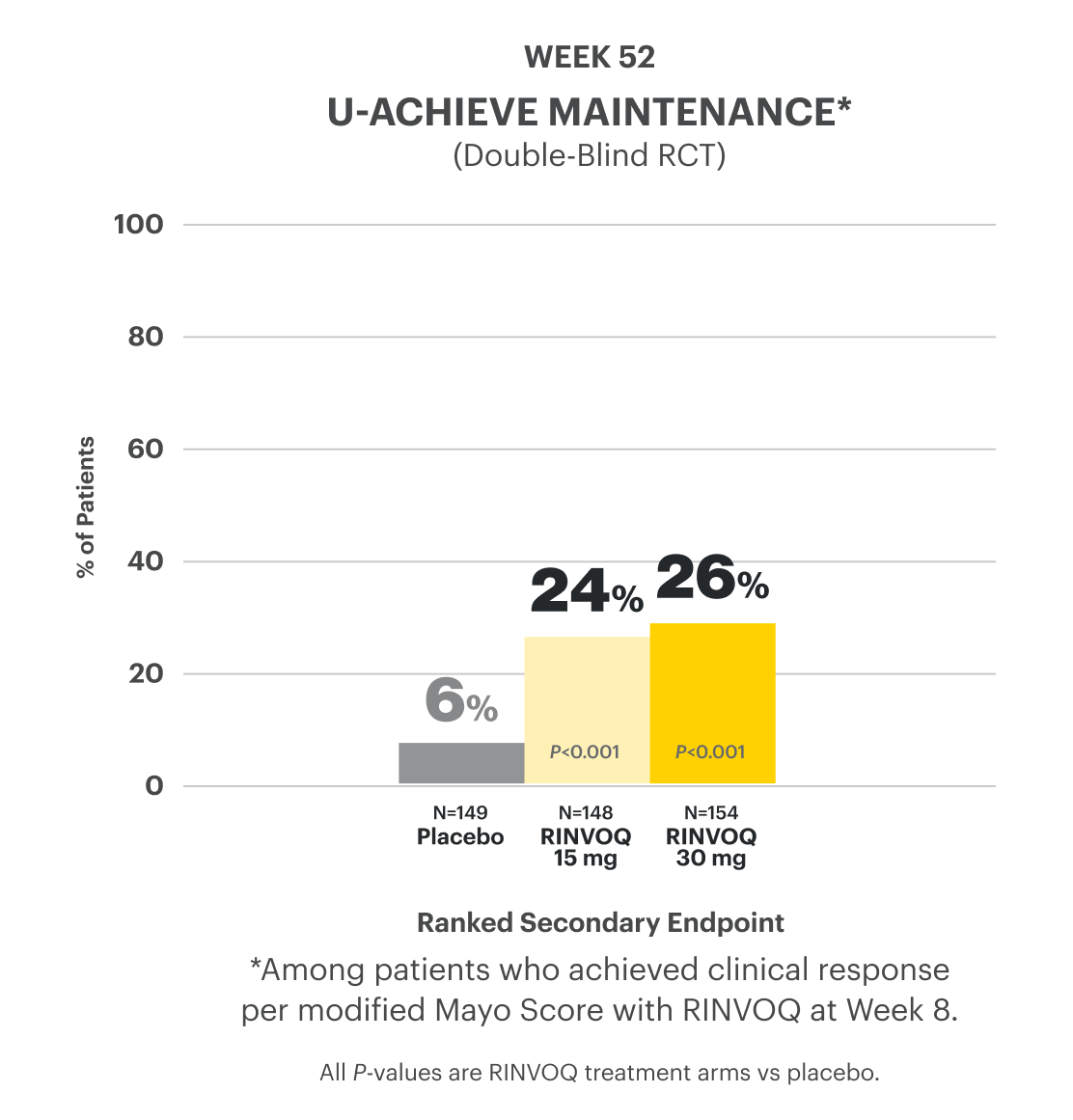
Corticosteroid-Free Clinical Remission at Week 521*
*Among patients who achieved remission at Week 8.
RECOMMENDED MAINTENANCE DOSING
The recommended maintenance dosage of RINVOQ is 15 mg once daily. A dose of 30 mg once daily may be considered for patients with refractory, severe, or extensive disease. Discontinue RINVOQ if an adequate therapeutic response is not achieved with the 30 mg dose.
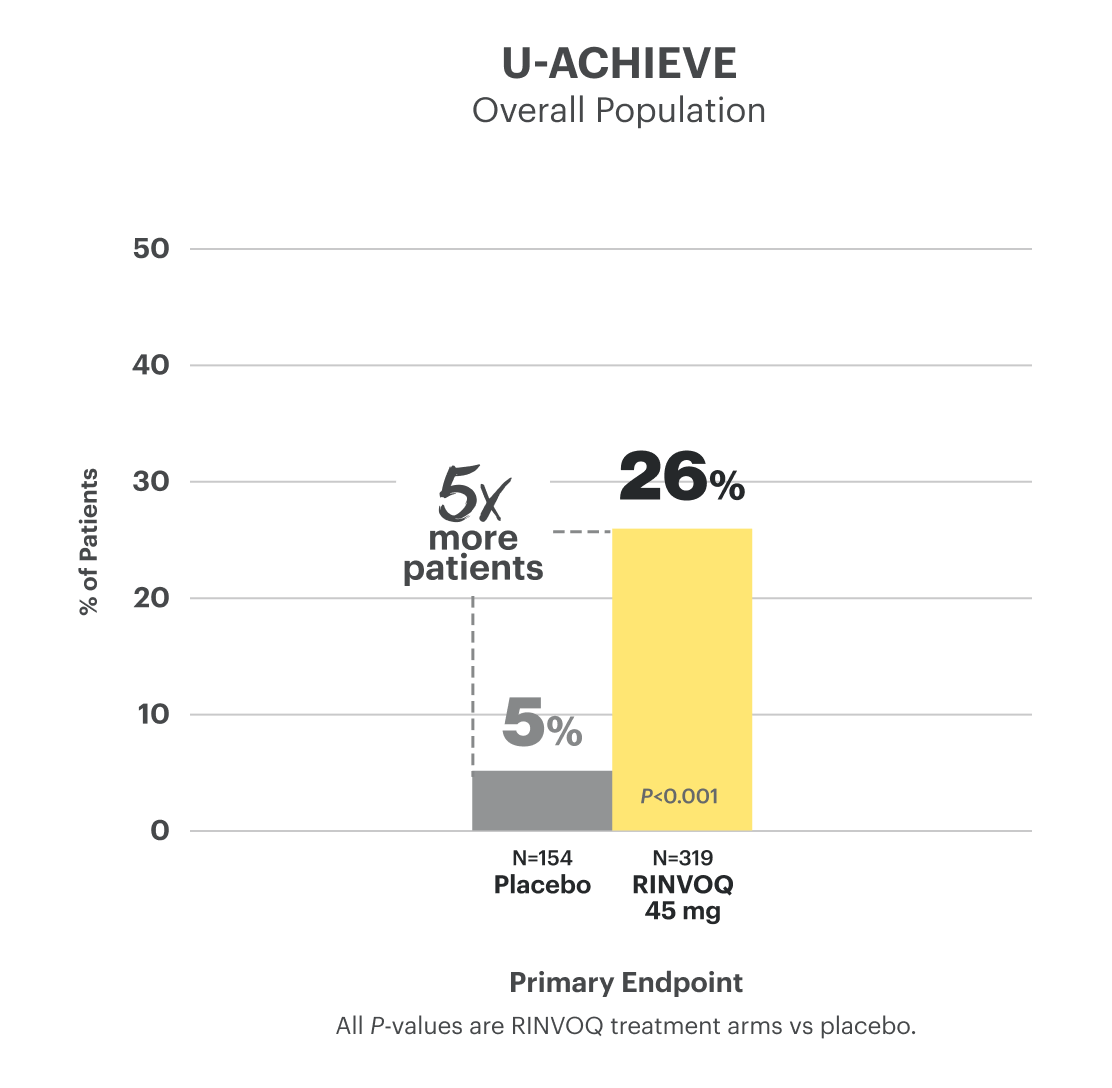
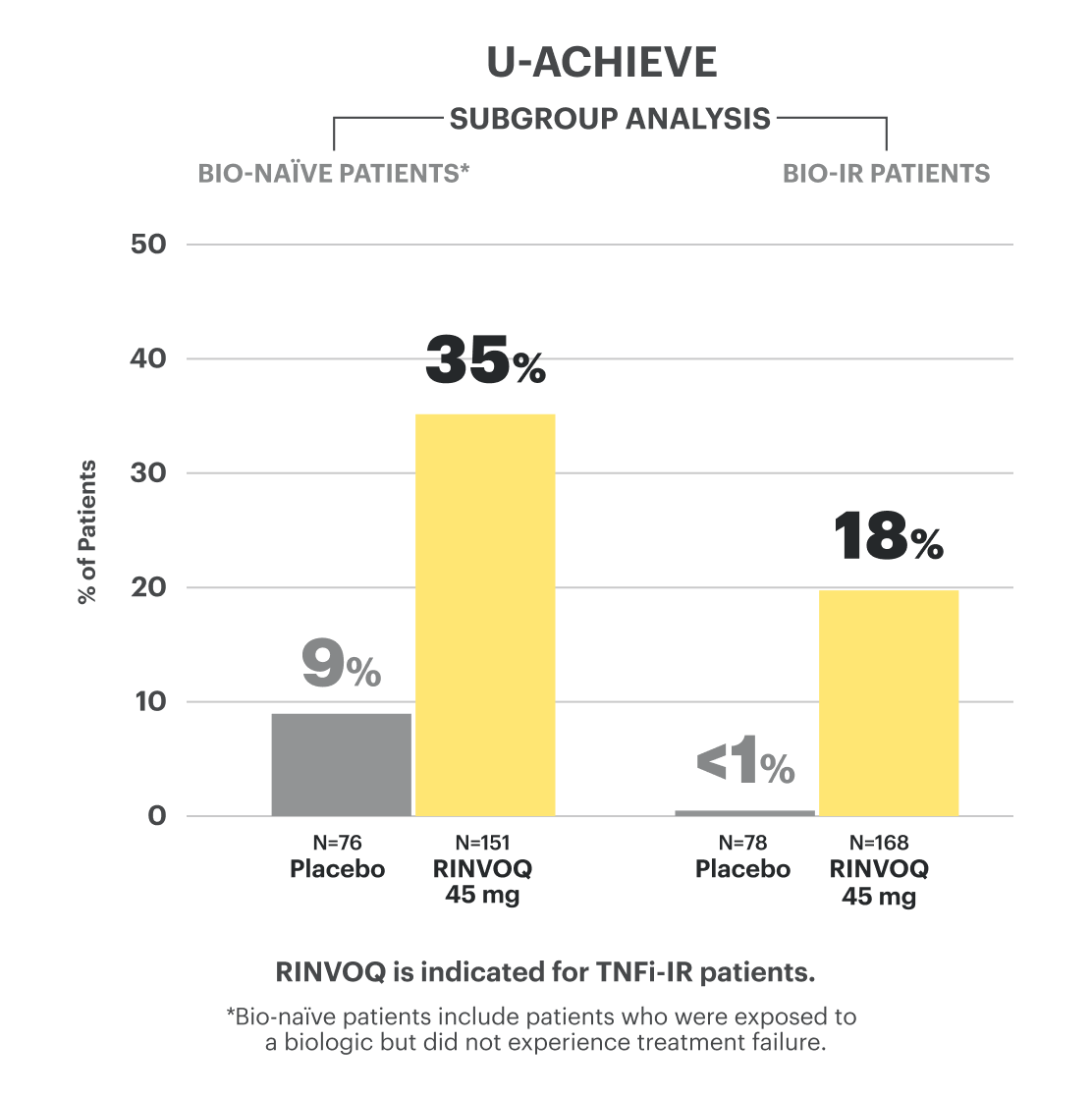
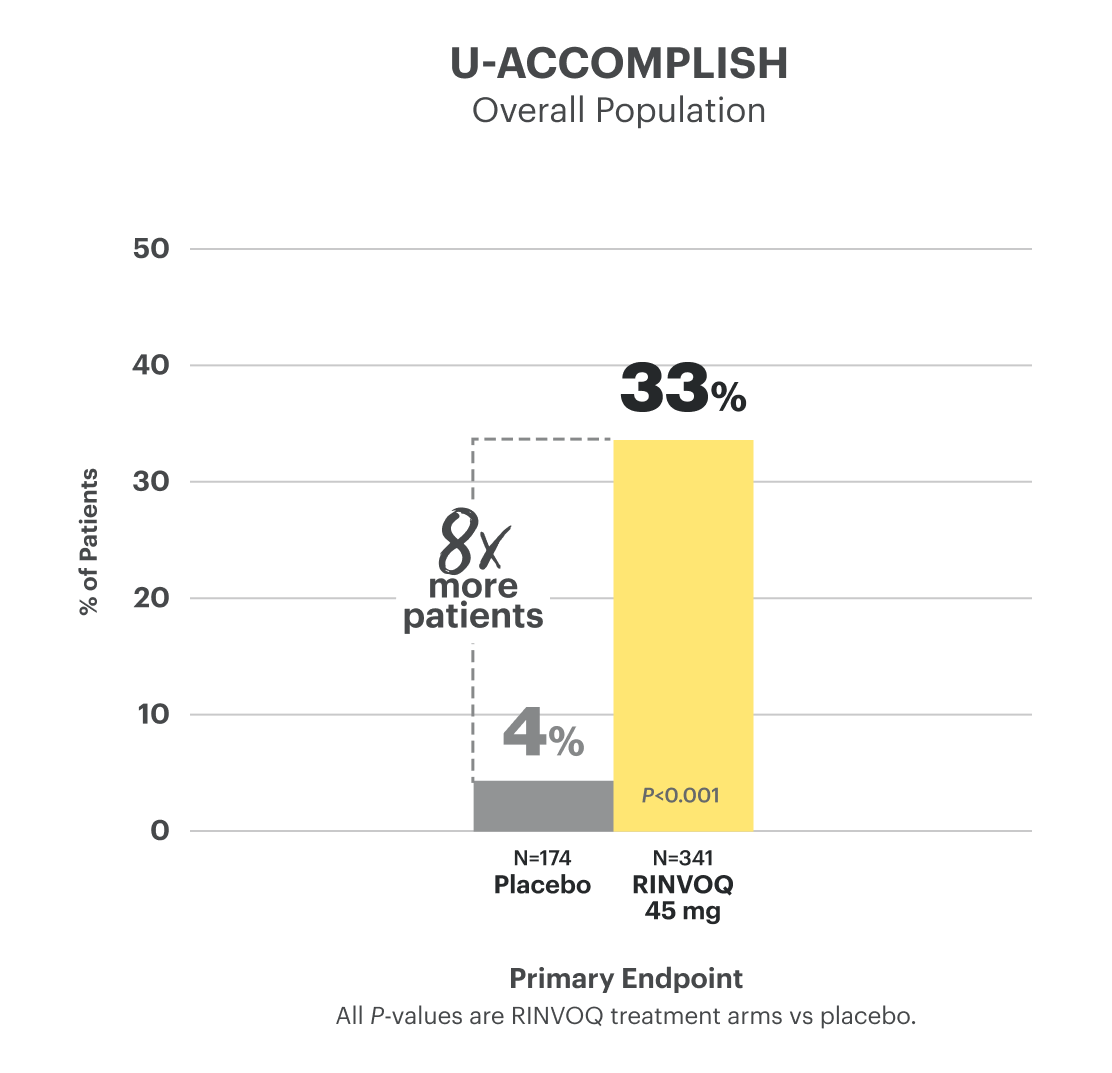
Clinical Remission at Week 81
RECOMMENDED MAINTENANCE DOSING
The recommended maintenance dosage of RINVOQ is 15 mg once daily. A dose of 30 mg may be considered for patients with refractory, severe or extensive disease. Discontinue if therapeutic response is not achieved with the 30 mg dose.
RECOMMENDED MAINTENANCE DOSING
The recommended maintenance dosage of RINVOQ is 15 mg once daily. A dose of 30 mg may be considered for patients with refractory, severe or extensive disease. Discontinue if therapeutic response is not achieved with the 30 mg dose.
Powerful Healing
at Weeks 8 and 52
Endoscopic & Histo‑endoscopic Mucosal Improvement Data
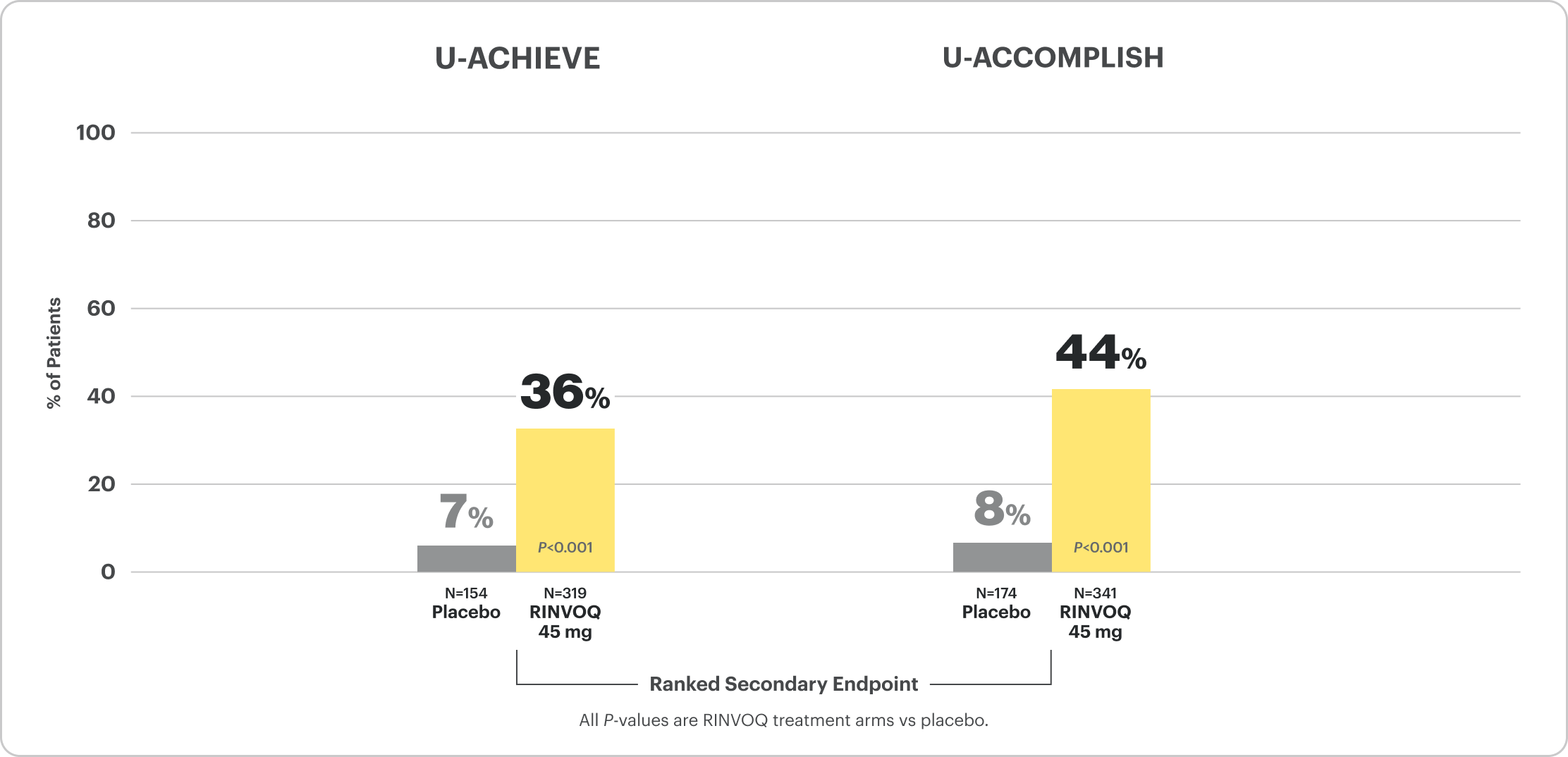
Endoscopic Improvement at Week 52 and Up to Week 1481,2
(Endoscopy subscore of 0 or 1, without friability)
RECOMMENDED MAINTENANCE DOSING
The recommended maintenance dosage of RINVOQ is 15 mg once daily. A dose of 30 mg once daily may be considered for patients with refractory, severe, or extensive disease. Discontinue RINVOQ if an adequate therapeutic response is not achieved with the 30 mg dose.
OLE LIMITATIONS: In an open-label extension (OLE), there is a potential for enrichment of the long-term data in the remaining patient populations since patients who are unable to tolerate or do not respond to the drug often drop out.
AO DISCLOSURE: In an as-observed (AO) analysis, missing visit data were excluded from calculations for that visit, which may increase the percent of responders. All observed data were used regardless of premature discontinuation of study drug or initiation of concomitant medications. The same patient may not have a response at each timepoint.

Patient baseline characteristics at induction include4:
70% Endoscopic Subscore 3
30% Endoscopic Subscore 2
†Bio-IR is defined as patients who have an inadequate response to, lose response to, or are intolerant to biologic therapy.
RECOMMENDED MAINTENANCE DOSING
The recommended maintenance dosage of RINVOQ is 15 mg once daily. A dose of 30 mg once daily may be considered for patients with refractory, severe, or extensive disease. Discontinue RINVOQ if an adequate therapeutic response is not achieved with the 30 mg dose.
OLE LIMITATIONS: In an open-label extension (OLE), there is a potential for enrichment of the long-term data in the remaining patient populations since patients who are unable to tolerate or do not respond to the drug often drop out.
AO DISCLOSURE: In an as-observed (AO) analysis, missing visit data were excluded from calculations for that visit, which may increase the percent of responders. All observed data were used regardless of premature discontinuation of study drug or initiation of concomitant medications. The same patient may not have a response at each timepoint.
Patient baseline characteristics at induction include4:
70% Endoscopic Subscore 3
30% Endoscopic Subscore 2
†Bio-IR is defined as patients who have an inadequate response to, lose response to, or are intolerant to biologic therapy.
RECOMMENDED MAINTENANCE DOSING
The recommended maintenance dosage of RINVOQ is 15 mg once daily. A dose of 30 mg once daily may be considered for patients with refractory, severe, or extensive disease. Discontinue RINVOQ if an adequate therapeutic response is not achieved with the 30 mg dose.
OLE LIMITATIONS: In an open-label extension (OLE), there is a potential for enrichment of the long-term data in the remaining patient populations since patients who are unable to tolerate or do not respond to the drug often drop out.
AO DISCLOSURE: In an as-observed (AO) analysis, missing visit data were excluded from calculations for that visit, which may increase the percent of responders. All observed data were used regardless of premature discontinuation of study drug or initiation of concomitant medications. The same patient may not have a response at each timepoint.
Patient baseline characteristics at induction include4:
70% Endoscopic Subscore 3
30% Endoscopic Subscore 2
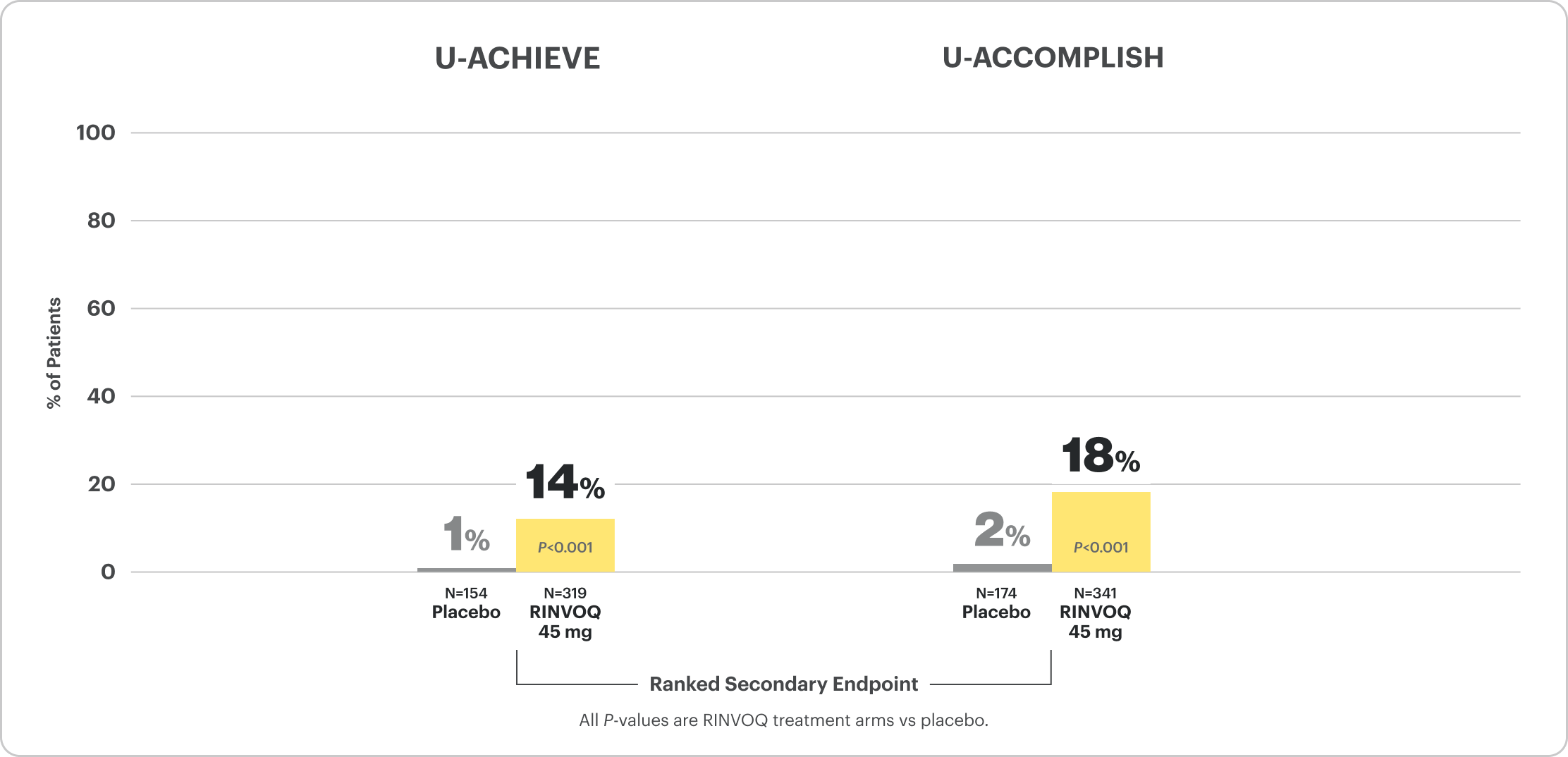
Endoscopic Remission at Week 52 and Up to Week 1481,2
(Endoscopy subscore of 0)
RECOMMENDED MAINTENANCE DOSING
The recommended maintenance dosage of RINVOQ is 15 mg once daily. A dose of 30 mg once daily may be considered for patients with refractory, severe, or extensive disease. Discontinue RINVOQ if an adequate therapeutic response is not achieved with the 30 mg dose.
OLE LIMITATIONS: In an open-label extension (OLE), there is a potential for enrichment of the long-term data in the remaining patient populations since patients who are unable to tolerate or do not respond to the drug often drop out.
AO DISCLOSURE: In an as-observed (AO) analysis, missing visit data were excluded from calculations for that visit, which may increase the percent of responders. All observed data were used regardless of premature discontinuation of study drug or initiation of concomitant medications. The same patient may not have a response at each timepoint.
†Bio-IR is defined as patients who have an inadequate response to, lose response to, or are intolerant to biologic therapy.
RECOMMENDED MAINTENANCE DOSING
The recommended maintenance dosage of RINVOQ is 15 mg once daily. A dose of 30 mg once daily may be considered for patients with refractory, severe, or extensive disease. Discontinue RINVOQ if an adequate therapeutic response is not achieved with the 30 mg dose.
OLE LIMITATIONS: In an open-label extension (OLE), there is a potential for enrichment of the long-term data in the remaining patient populations since patients who are unable to tolerate or do not respond to the drug often drop out.
AO DISCLOSURE: In an as-observed (AO) analysis, missing visit data were excluded from calculations for that visit, which may increase the percent of responders. All observed data were used regardless of premature discontinuation of study drug or initiation of concomitant medications. The same patient may not have a response at each timepoint.

Endoscopy Subscore=0
†Bio-IR is defined as patients who have an inadequate response to, lose response to, or are intolerant to biologic therapy.
RECOMMENDED MAINTENANCE DOSING
The recommended maintenance dosage of RINVOQ is 15 mg once daily. A dose of 30 mg once daily may be considered for patients with refractory, severe, or extensive disease. Discontinue RINVOQ if an adequate therapeutic response is not achieved with the 30 mg dose.
OLE LIMITATIONS: In an open-label extension (OLE), there is a potential for enrichment of the long-term data in the remaining patient populations since patients who are unable to tolerate or do not respond to the drug often drop out.
AO DISCLOSURE: In an as-observed (AO) analysis, missing visit data were excluded from calculations for that visit, which may increase the percent of responders. All observed data were used regardless of premature discontinuation of study drug or initiation of concomitant medications. The same patient may not have a response at each timepoint.
Endoscopy Subscore=0
Histo-endoscopic Mucosal Improvement1
(Endoscopic subscore of 0 or 1, without friability and histologic improvement with Geboes score ≤3.1)
*Among patients who achieved clinical response per modified Mayo Score with RINVOQ at Week 8.
The relationship between this endpoint to disease progression and long-term outcomes was not evaluated.
RECOMMENDED MAINTENANCE DOSING
The recommended maintenance dosage of RINVOQ is 15 mg once daily. A dose of 30 mg once daily may be considered for patients with refractory, severe, or extensive disease. Discontinue RINVOQ if an adequate therapeutic response is not achieved with the 30 mg dose.
The relationship between this endpoint to disease progression and long-term outcomes was not evaluated.
RECOMMENDED MAINTENANCE DOSING
The recommended maintenance dosage of RINVOQ is 15 mg once daily. A dose of 30 mg once daily may be considered for patients with refractory, severe, or extensive disease. Discontinue RINVOQ if an adequate therapeutic response is not achieved with the 30 mg dose.
Endoscopic Outcomes at Week 81
RECOMMENDED MAINTENANCE DOSING
The recommended maintenance dosage of RINVOQ is 15 mg once daily. A dose of 30 mg once daily may be considered for patients with refractory, severe, or extensive disease. Discontinue RINVOQ if an adequate therapeutic response is not achieved with the 30 mg dose.
Patient baseline characteristics at induction include4:
70% Endoscopic Subscore 3
30% Endoscopic Subscore 2
RECOMMENDED MAINTENANCE DOSING
The recommended maintenance dosage of RINVOQ is 15 mg once daily. A dose of 30 mg once daily may be considered for patients with refractory, severe, or extensive disease. Discontinue RINVOQ if an adequate therapeutic response is not achieved with the 30 mg dose.
Patient baseline characteristics at induction include4:
70% Endoscopic Subscore 3
30% Endoscopic Subscore 2
Safety Considerations
Serious Infections: RINVOQ-treated patients are at increased risk of serious bacterial (including tuberculosis [TB]), fungal, viral, and opportunistic infections leading to hospitalization or death. Most patients who developed these infections were taking concomitant immunosuppressants, such as methotrexate or corticosteroids.
Mortality: A higher rate of all-cause mortality, including sudden cardiovascular (CV) death, was observed with a Janus kinase inhibitor (JAKi) in a study comparing another JAKi with tumor necrosis factor (TNF) blockers in rheumatoid arthritis (RA) patients ≥50 years with ≥1 CV risk factor.
Malignancies: Malignancies have occurred in RINVOQ-treated patients. A higher rate of lymphomas and lung cancer (in current or past smokers) was observed with another JAKi when compared with TNF blockers in RA patients.
Major Adverse Cardiovascular Events: A higher rate of CV death, myocardial infarction, and stroke was observed with a JAKi in a study comparing another JAKi with TNF blockers in RA patients ≥50 years with ≥1 CV risk factor. History of smoking increases risk.
Thromboses: Deep venous thrombosis, pulmonary embolism, and arterial thrombosis have occurred in patients treated for inflammatory conditions with JAK inhibitors, including RINVOQ. A higher rate of thrombosis was observed with another JAKi when compared with TNF blockers in RA patients.
Hypersensitivity: RINVOQ is contraindicated in patients with hypersensitivity to RINVOQ or its excipients.
Other Serious Adverse Reactions: Hypersensitivity Reactions, Gastrointestinal Perforations, Laboratory Abnormalities, and Embryo-Fetal Toxicity.
Rapid Relief
of Rectal Bleeding and Stool Frequency at Week 2
Clinical Response at Weeks 2, 4, 6, and 85
Composite of Rectal Bleeding and Stool Frequency Subscores

CLINICAL RESPONSE AT WEEK 2:
- U-ACHIEVE Induction: 60% on RINVOQ 45 mg vs 27% on placebo (P<0.001)4
- U-ACCOMPLISH Induction: 63% on RINVOQ 45 mg vs 26% on placebo (P<0.001)4
DATA LIMITATIONS: The pre-specified integrated analysis for Clinical Response at Week 2 and over time is considered supportive of the efficacy results obtained from the individual studies and is intended to be interpreted within this context. No multiplicity adjustment was performed; thus, no statistical inferences can be made.
Patient Symptoms Data by Day
Rectal Bleeding Subscore (RBS) Data by Day6
(Daily Patient Diary Data)
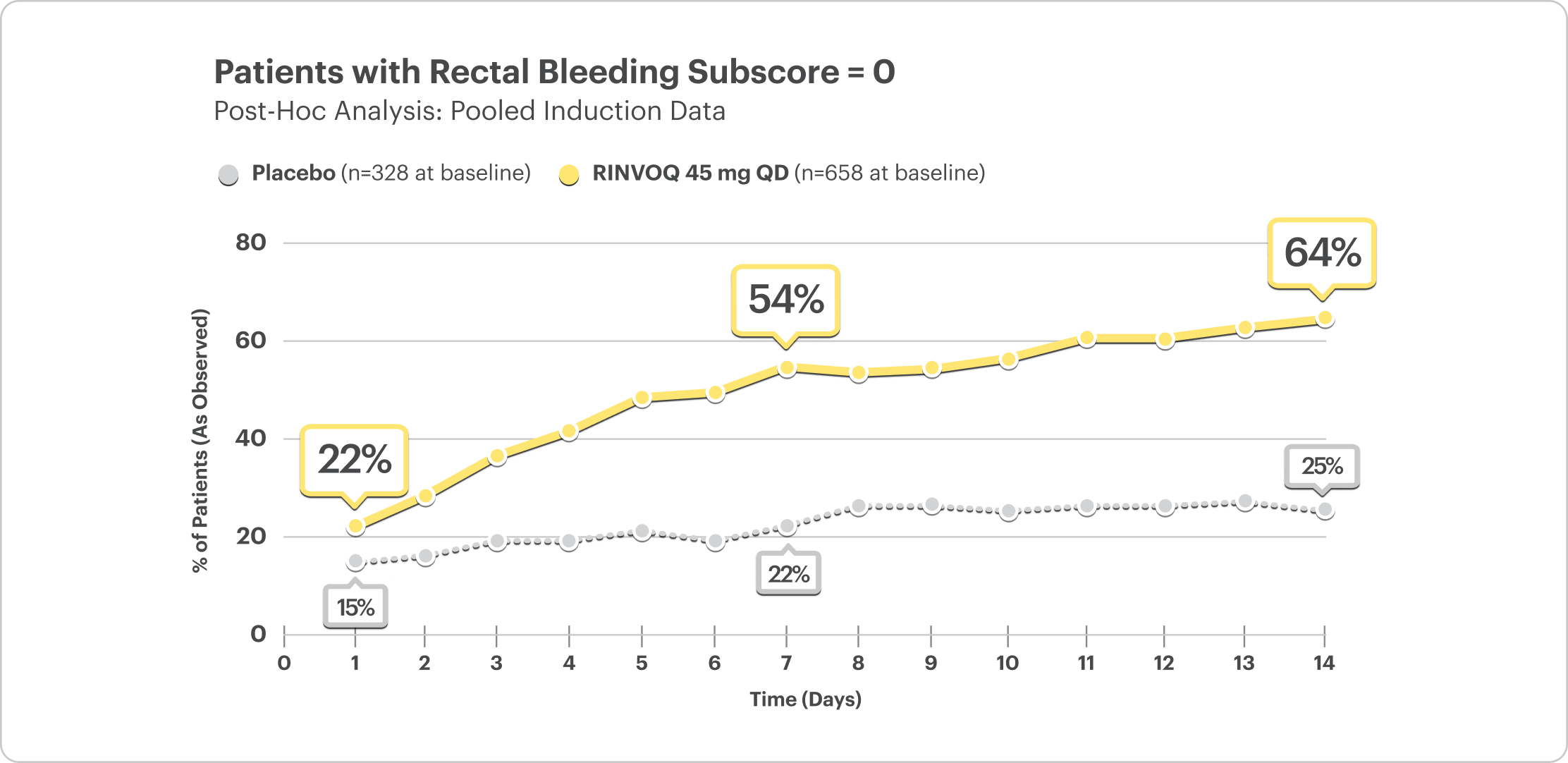
DATA LIMITATIONS: Post hoc analyses were not adjusted for multiplicity; thus, no statistical inferences can be made. These analyses utilized an as‑observed approach and did not impute values for missing evaluations.
- At Day 1, 22% of patients on RINVOQ 45 mg reported no rectal bleeding vs 15% on placebo6
- At Week 1, 54% of patients on RINVOQ 45 mg reported no rectal bleeding vs 22% on placebo6
Stool Frequency Subscore (SFS) Data by Day6
(Daily Patient Diary Data)
Patients with a reduction in stool frequency subscore ≤1 point
Post Hoc Analysis: Pooled Induction Data
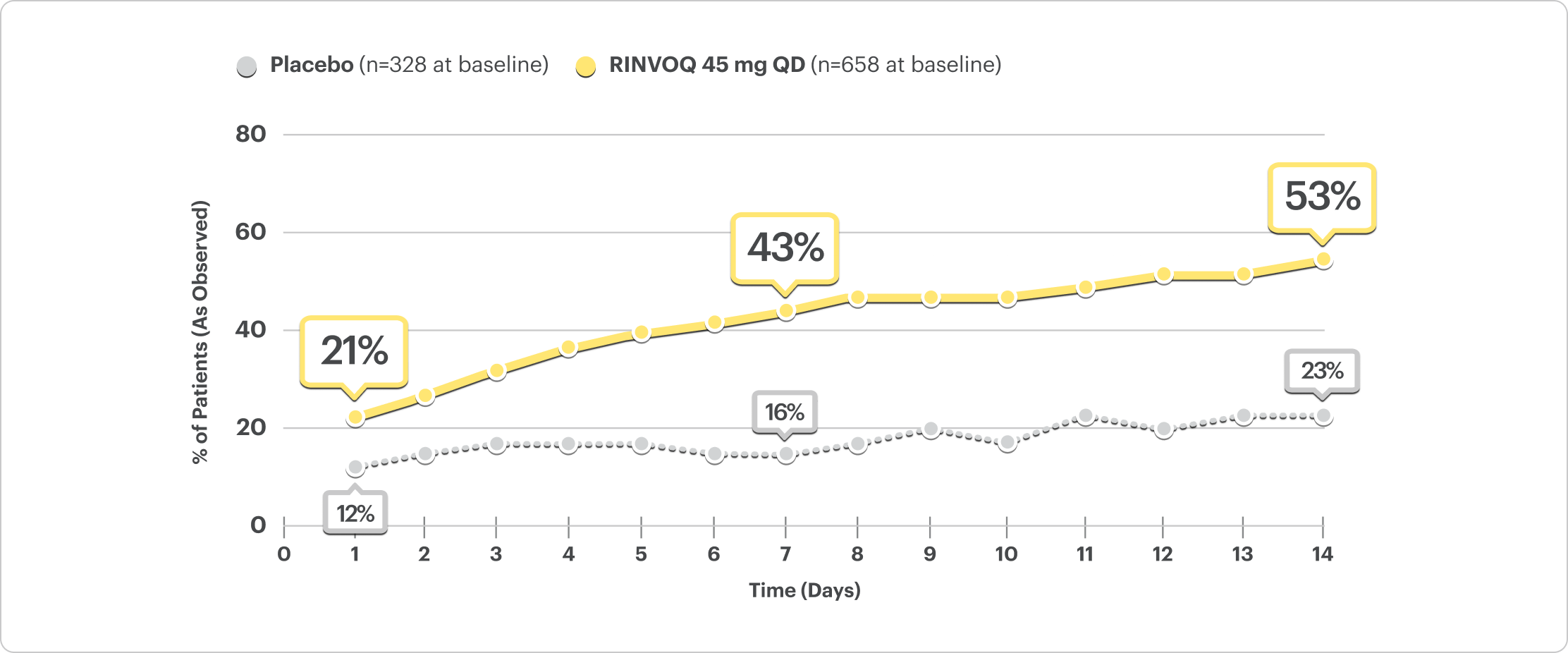
DATA LIMITATIONS: Post hoc analyses were not adjusted for multiplicity; thus, no statistical inferences can be made. These analyses utilized an as‑observed approach and did not impute values for missing evaluations.
- At Day 1, 21% of patients on RINVOQ 45 mg reported a reduction in stool frequency vs 12% on placebo6
- At Week 1, 43% of patients on RINVOQ 45 mg reported a reduction in stool frequency vs 16% on placebo6
No Bowel Urgency Data by Day6
(Daily Patient Diary Data)
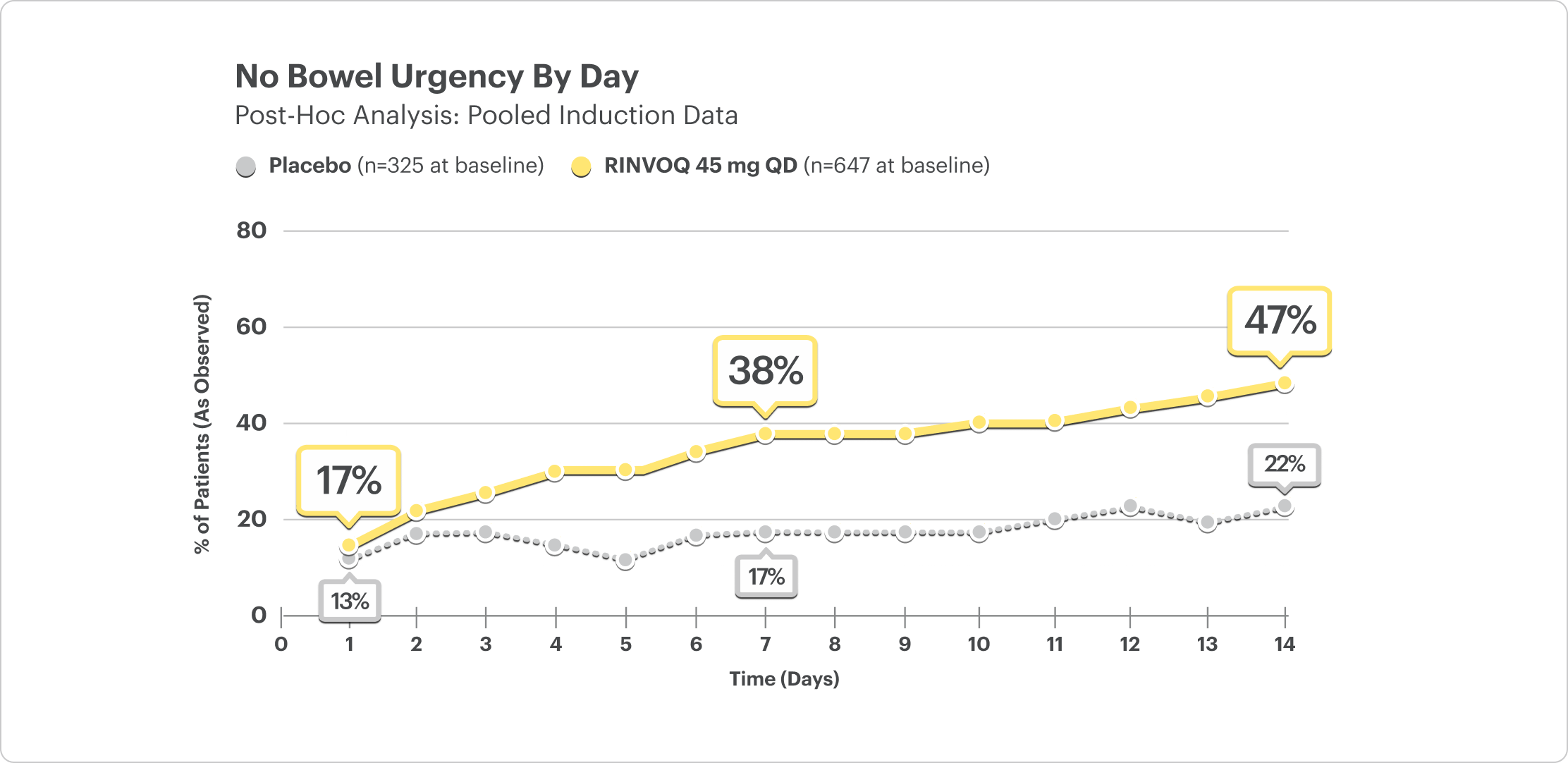
In the induction studies, a greater proportion of patients treated with RINVOQ 45 mg once daily compared to placebo had no bowel urgency (U‑ACHIEVE: 48% vs 21%, U‑ACCOMPLISH: 54% vs 26%) at Week 8.1
DATA LIMITATIONS: Post hoc analyses were not adjusted for multiplicity; thus, no statistical inferences can be made. These analyses utilized an as‑observed approach and did not impute values for missing evaluations.
- At Day 1, 17% of patients on RINVOQ 45 mg reported no bowel urgency vs 13% on placebo6
- At Week 1, 38% of patients on RINVOQ 45 mg reported no bowel urgency vs 17% on placebo6
Fecal Calprotectin Reduction at Weeks 2 and 87
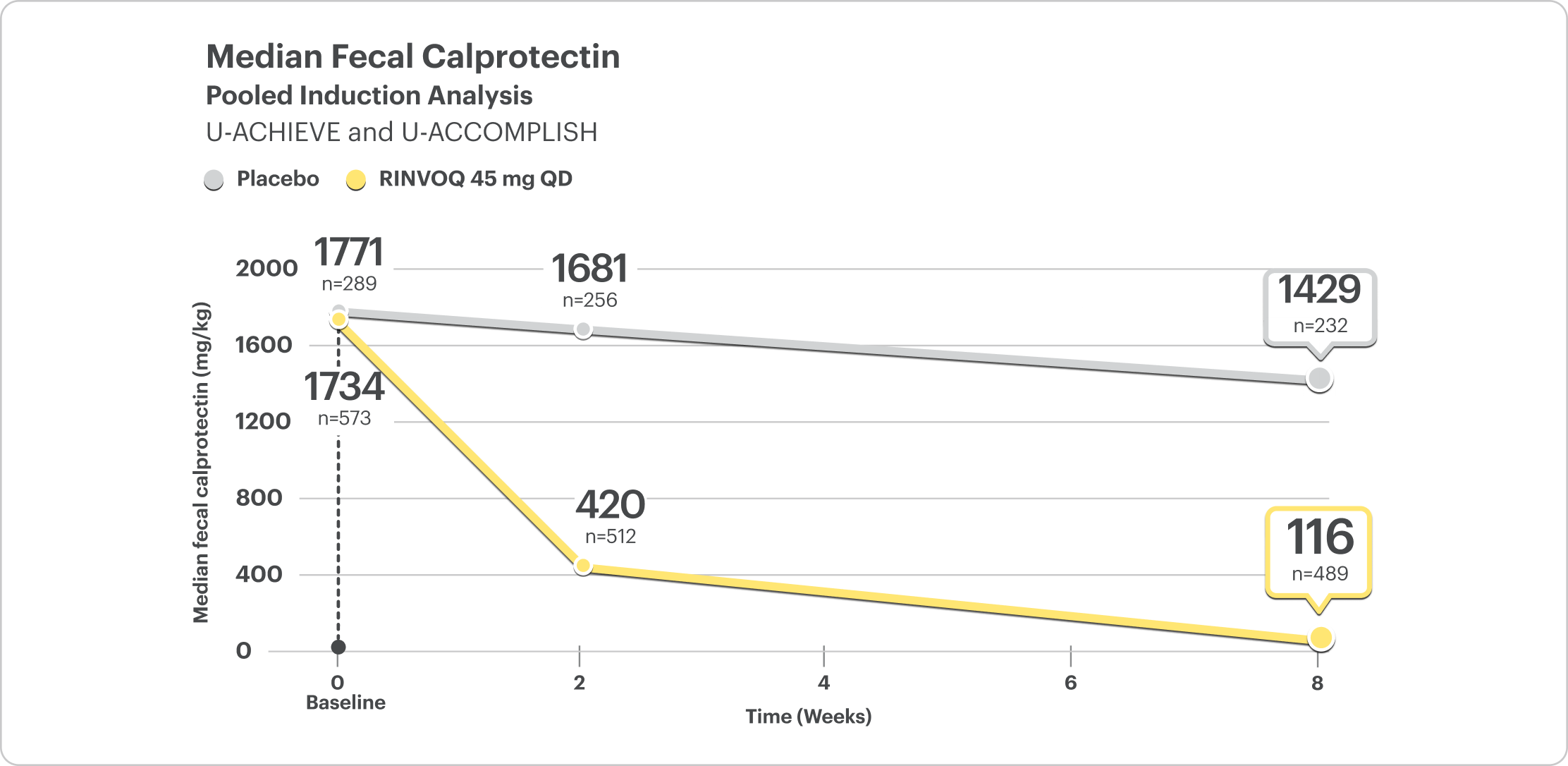
DATA LIMITATIONS: Fecal calprotectin <150 mg/kg at Week 2 and Week 8 of the integrated induction data was a prespecified analysis. Change from baseline in median fecal calprotectin at Week 2 and Week 8 was a post hoc analysis. Neither of these analyses were adjusted for multiplicity; thus, no statistical inferences can be made.
Fecal calprotectin is not validated as a biomarker to monitor disease progression.
FECAL CALPROTECTIN <150 MG/KG
- At Week 2, 30% of patients on RINVOQ 45 mg had FC <150 mg/kg compared to 5% on placebo8
- At Week 8, 46% of patients on RINVOQ 45 mg had FC <150 mg/kg compared to 8% on placebo8
Interested in the safety data for RINVOQ?
See RINVOQ’s safety data across clinical trials