DURABLE REMISSION
WITH RAPID STEROID REDUCTION
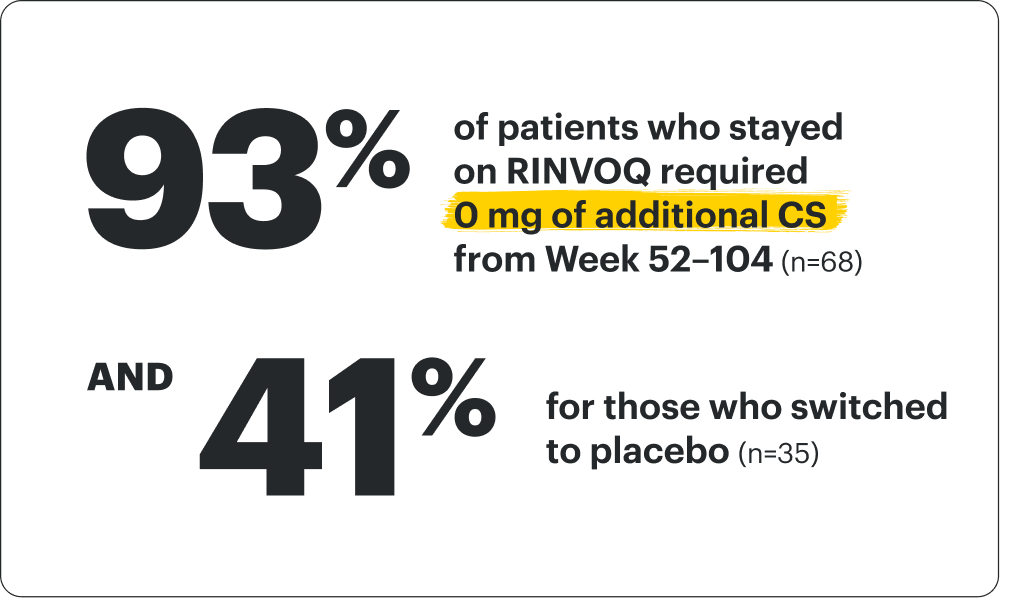
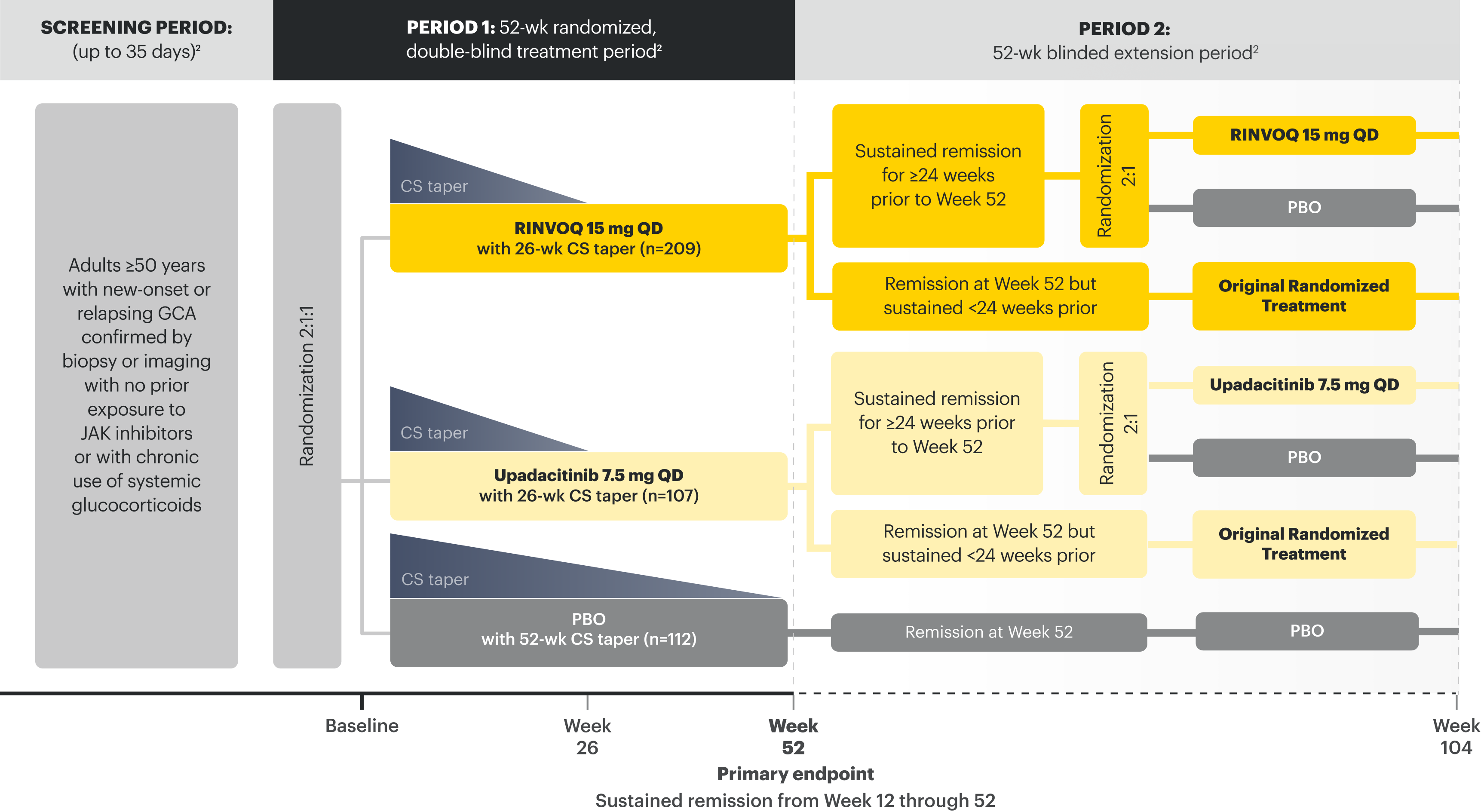
GCA patients on a 26-wk CS taper achieved sustained remission from Week 12 through 52 (primary endpoint). In patients who sustained remission from Week 28–52 with RINVOQ, remission rates were observed out to 2 years.1-3
CS=corticosteroid; GCA=giant cell arteritis.
INDICATION
RINVOQ is indicated for the treatment of adults with giant cell arteritis (GCA).
Limitations of Use: RINVOQ is not recommended for use in combination with other Janus kinase (JAK) inhibitors, biologic disease-modifying antirheumatic drugs (bDMARDs), or with potent immunosuppressants such as azathioprine and cyclosporine.
NRI Data From SELECT-GCA1,2
RINVOQ 15 mg + 26-wk CS taper (n=209), placebo + 52-wk CS taper (n=112)
Sustained Remission | PRIMARY ENDPOINT
46% RINVOQ vs 29% placebo + 52-wk CS taper from Week 12 through 52*
*P=0.002.
SELECT-GCA1,2: 52-wk, randomized, double-blind, placebo-controlled study of 428 adult patients age 50+ with GCA. Patients were randomized to receive RINVOQ 15 mg + 26-wk CS taper or placebo + 52-wk CS taper.
Sustained remission: Absence of GCA signs and symptoms from Week 12 through 52 and adherence to the protocol-defined CS-taper regimen.
Please see Important Safety Information, including BOXED WARNING on Serious Infections, Mortality, Malignancies, Major Adverse Cardiovascular Events, and Thrombosis, below.
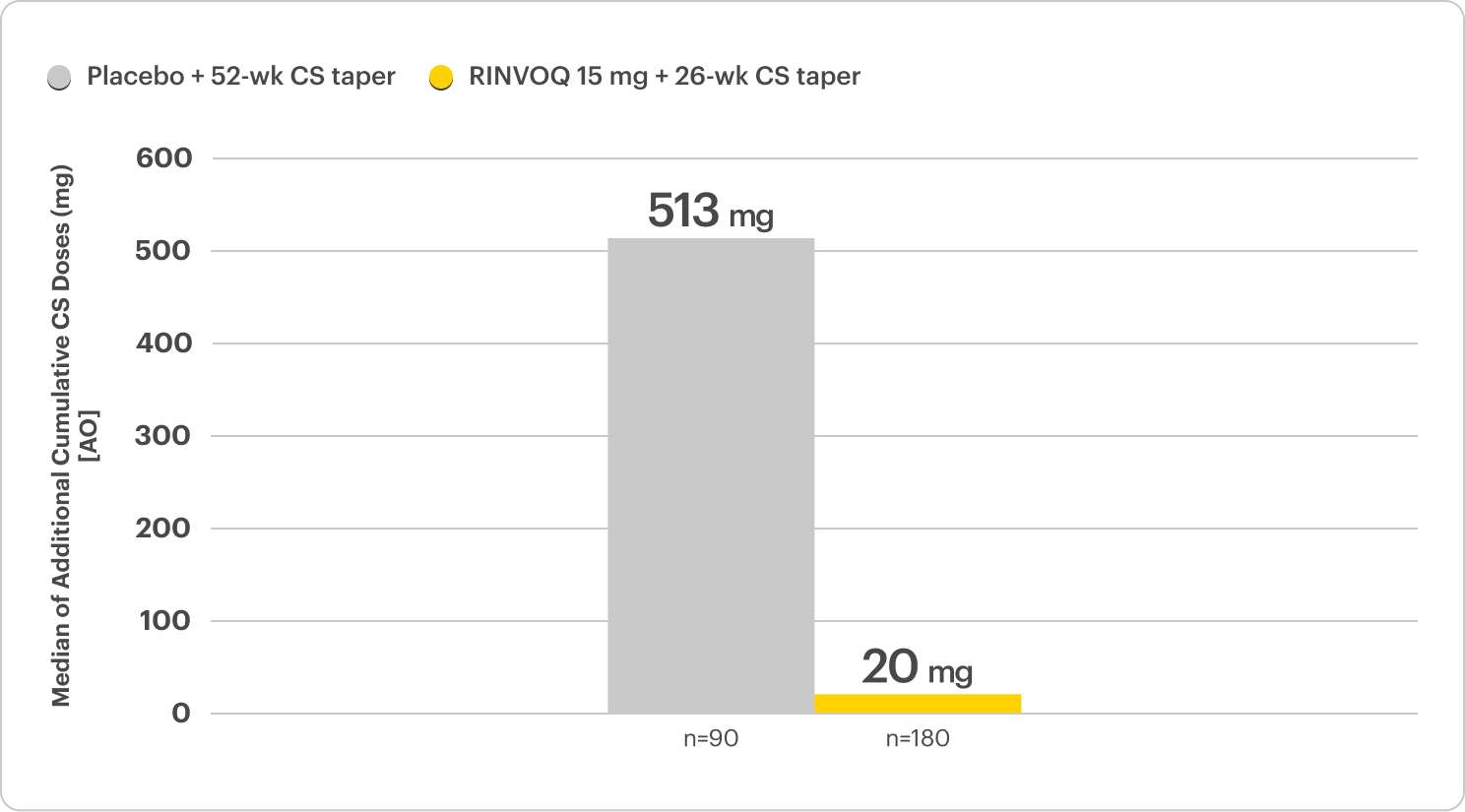
Rapid and Substantial Steroid Reduction
40% less cumulative steroid exposure with most patients off steroids in half the time
on RINVOQ 15 mg + 26-wk CS taper vs placebo + 52-wk CS taper2,4
SELECT-GCA Period 1 (Week 0–52)
ALL DATA ARE AS OBSERVED CASES
Median Cumulative CS Exposure

At Week 52, a substantially lower cumulative CS dose was observed in the RINVOQ 15 mg + 26-wk CS-taper arm.
The cumulative CS exposure includes all CS use during the 52 weeks of the trial. This includes the CS dose per protocol and above protocol.
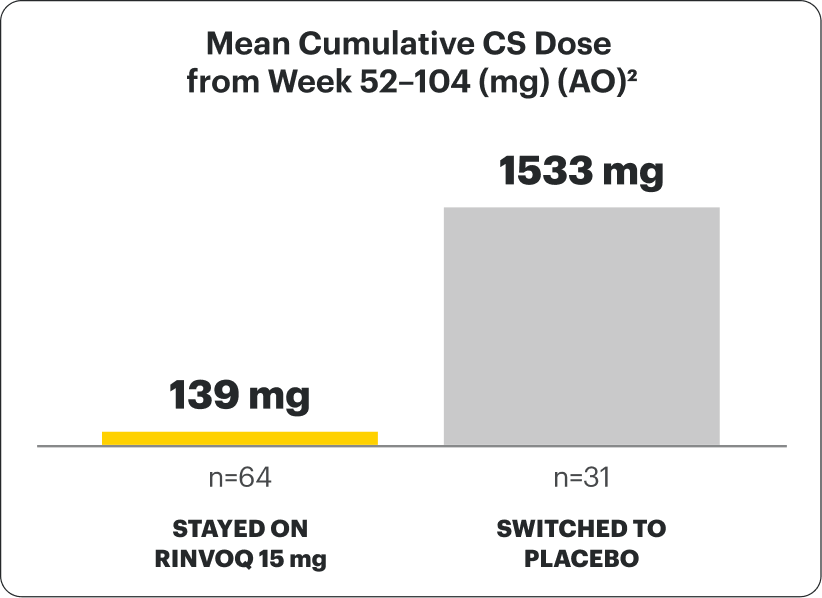
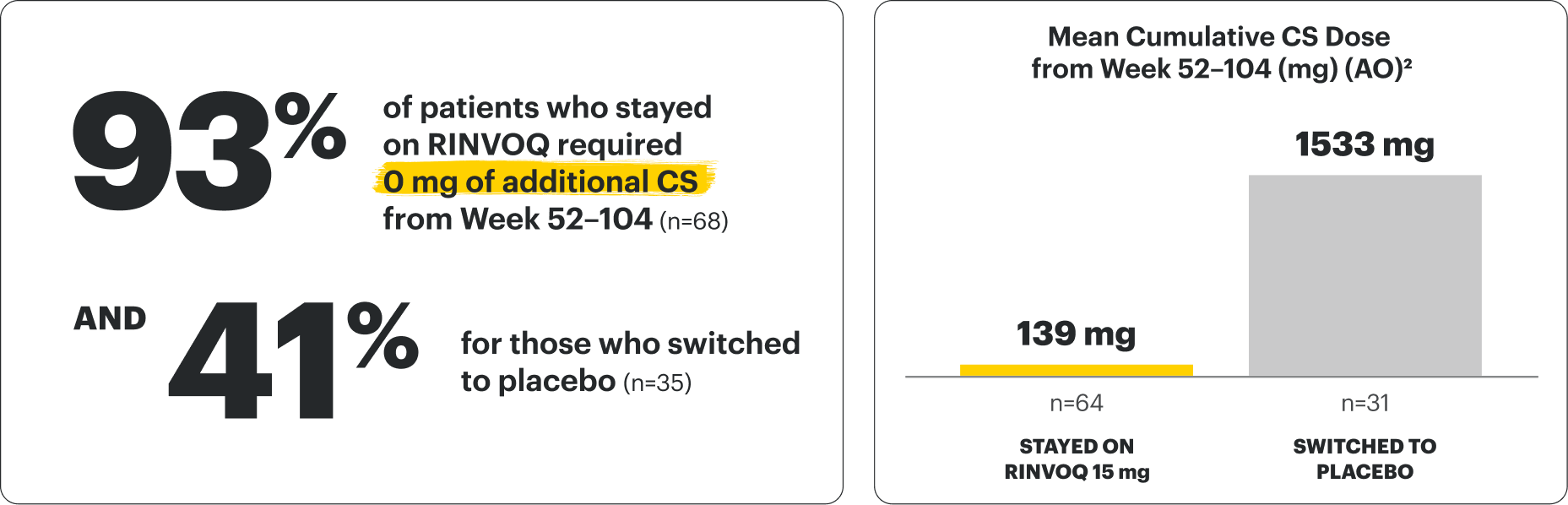
SEE HOW MANY PATIENTS WERE EXPOSED TO CS FROM WEEK 52–104
DATA LIMITATIONS: Data not labeled as ranked secondary endpoints were prespecified nonranked endpoints not controlled for multiplicity; therefore, treatment differences could represent chance findings. No conclusions regarding these comparisons can be made.
Steroid-free Complete Remission Achieved at 1 Year, With Rates Observed
Out to 2 Years
Steroid-free remission achieved in a significantly higher proportion of patients at 1 year2,4
SELECT-GCA Period 1
NRI-MI
Complete Remission
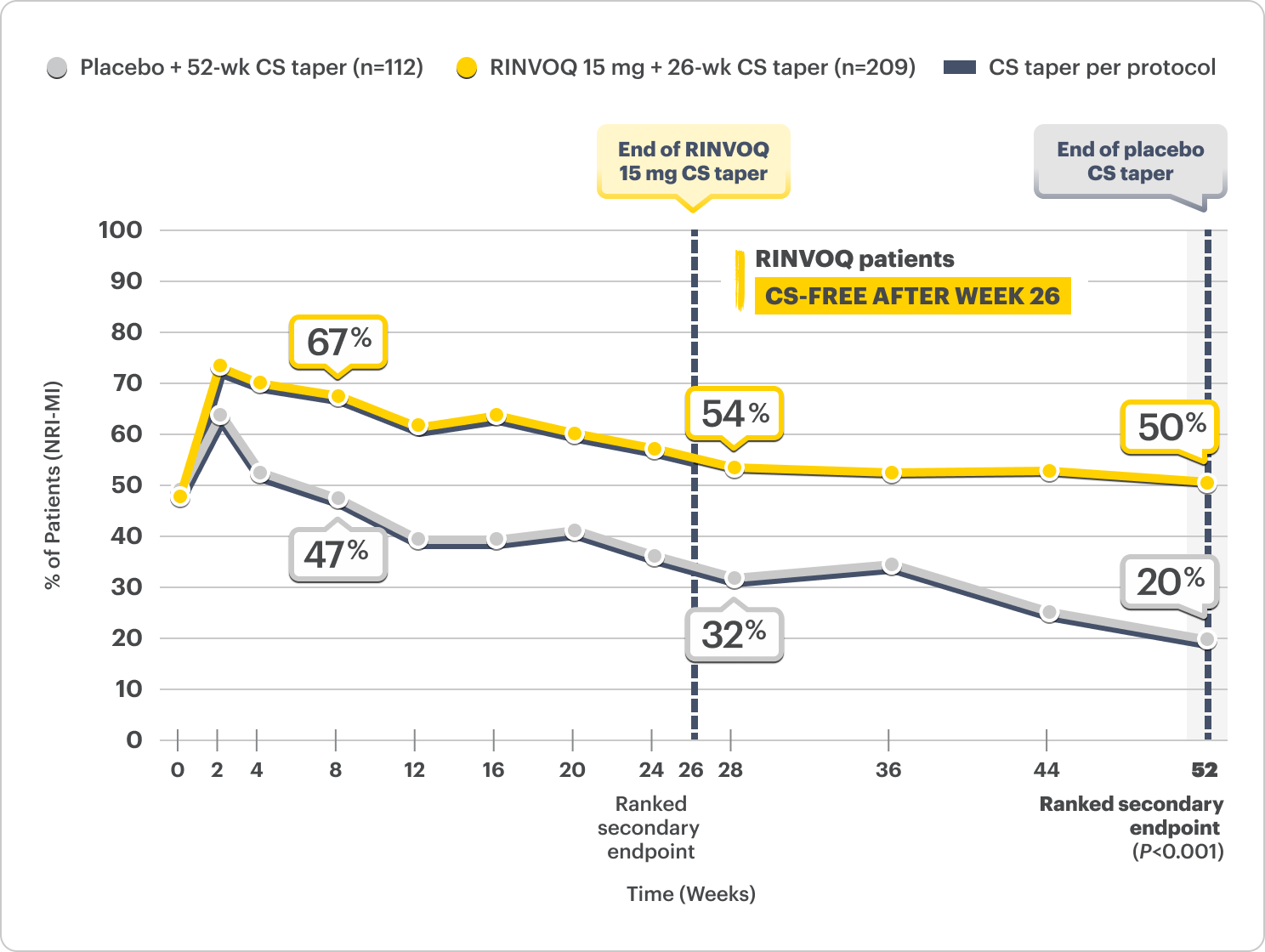
Defined as achieving all of the following:
- NO GCA signs and symptoms
- NO additional steroids above protocol-defined CS-taper regimen
- Normalization of ESR and hsCRP
DATA LIMITATIONS: Data not labeled as ranked secondary endpoints were prespecified nonranked endpoints not controlled for multiplicity; therefore, treatment differences could represent chance findings. No conclusions regarding these comparisons can be made.
Steroid-free remission rates observed out to 2 years6,7
SELECT-GCA Period 2
Patients with sustained remission on RINVOQ from Week 28–52
NRI-MI
Complete Remission
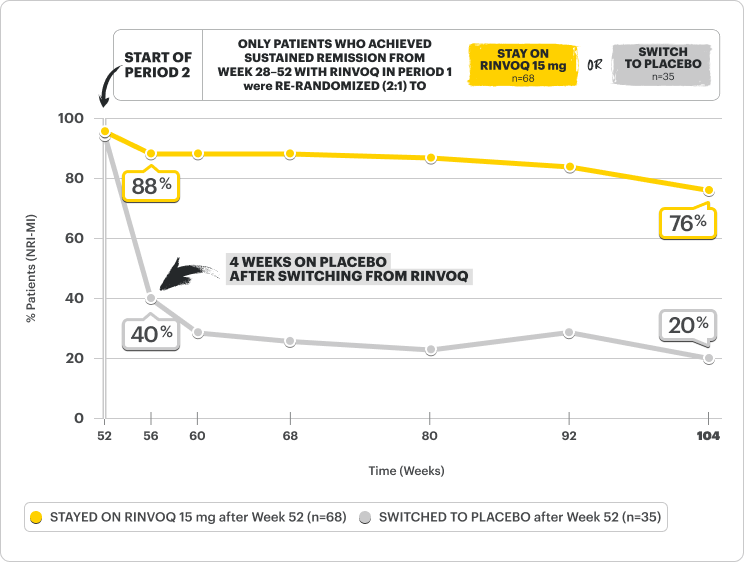
Defined as achieving all of the following:
- NO GCA signs and symptoms
- NO steroid use
- Normalization of ESR and hsCRP
DATA LIMITATIONS: Data were prespecified nonranked endpoints not controlled for multiplicity; therefore, treatment differences could represent chance findings. No conclusions regarding these comparisons can be made.
Safety Considerations
Serious Infections: RINVOQ-treated patients are at increased risk of serious bacterial (including tuberculosis [TB]), fungal, viral, and opportunistic infections leading to hospitalization or death. Most patients who developed these infections were taking concomitant immunosuppressants, such as methotrexate or corticosteroids.
Mortality: A higher rate of all-cause mortality, including sudden cardiovascular (CV) death, was observed with a Janus kinase inhibitor (JAKi) in a study comparing another JAKi with tumor necrosis factor (TNF) blockers in rheumatoid arthritis (RA) patients ≥50 years with ≥1 CV risk factor.
Malignancies: Malignancies have occurred in RINVOQ-treated patients. A higher rate of lymphomas and lung cancer (in current or past smokers) was observed with another JAKi when compared with TNF blockers in RA patients.
Major Adverse Cardiovascular Events: A higher rate of CV death, myocardial infarction, and stroke was observed with a JAKi in a study comparing another JAKi with TNF blockers in RA patients ≥50 years with ≥1 CV risk factor. History of smoking increases risk.
Thromboses: Deep venous thrombosis, pulmonary embolism, and arterial thrombosis have occurred in patients treated for inflammatory conditions with JAK inhibitors, including RINVOQ. A higher rate of thrombosis was observed with another JAKi when compared with TNF blockers in RA patients.
Hypersensitivity: RINVOQ is contraindicated in patients with hypersensitivity to RINVOQ or its excipients.
Other Serious Adverse Reactions: Hypersensitivity Reactions, Gastrointestinal Perforations, Laboratory Abnormalities, and Embryo-Fetal Toxicity.
Interested in the safety data for RINVOQ?
See RINVOQ’s safety data across clinical trials